

The Immunology of Multisystem Inflammatory Syndrome in Children with COVID-19
- PMID: 32966765
- PMCID: PMC7474869
- DOI: 10.1016/j.cell.2020.09.016
The Immunology of Multisystem Inflammatory Syndrome in Children with COVID-19
Abstract
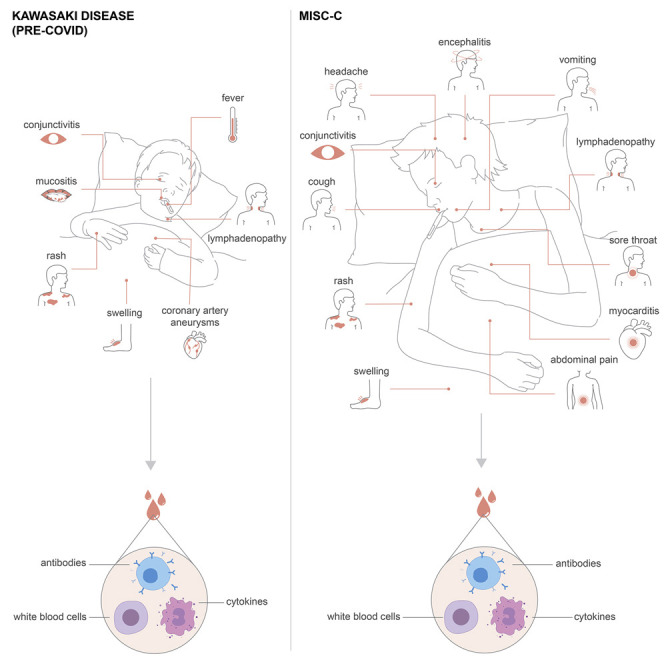
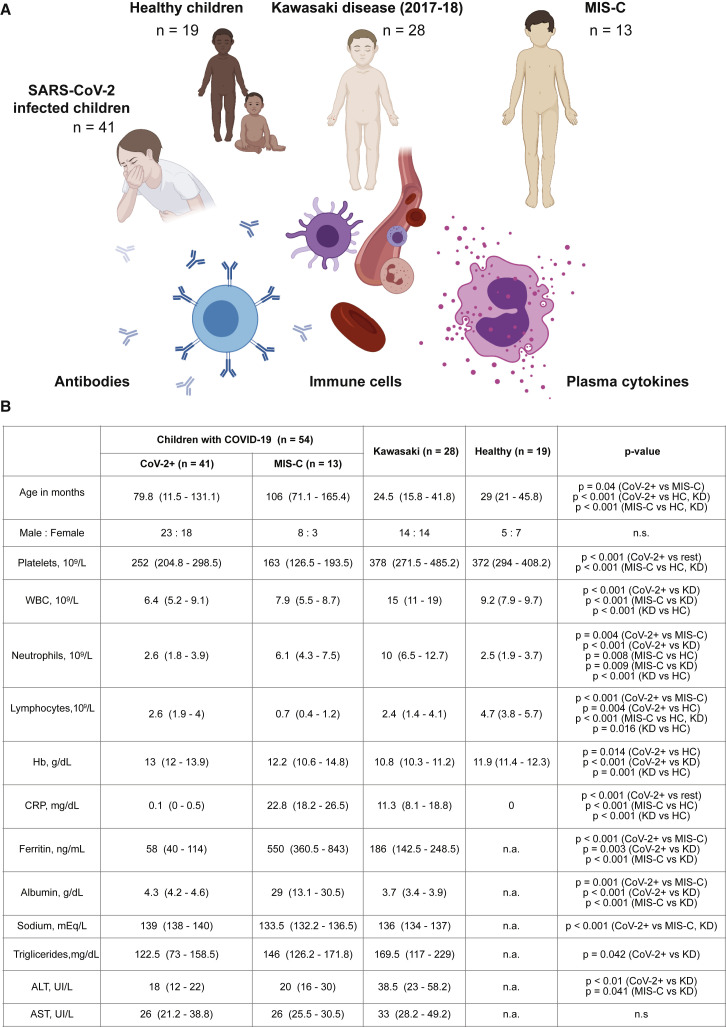
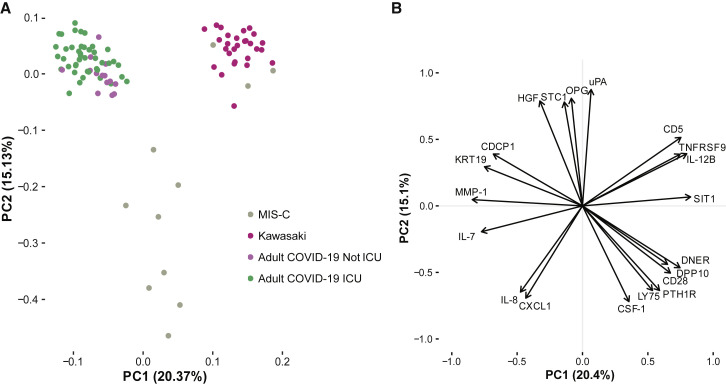
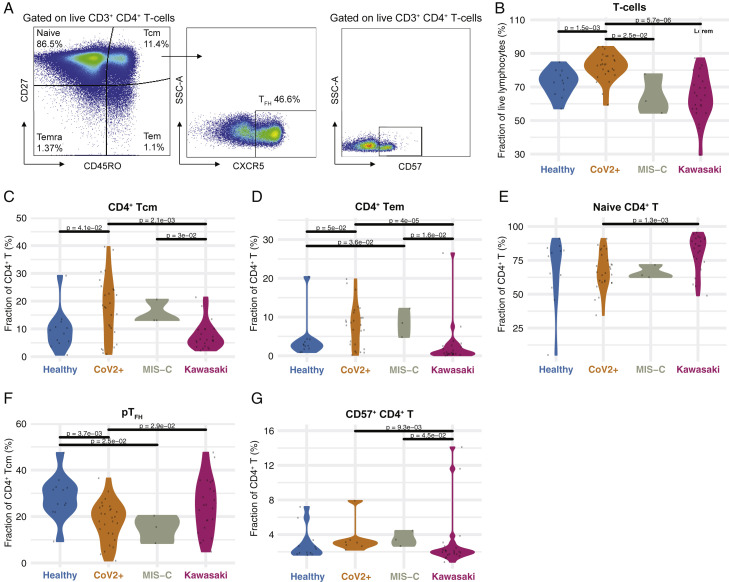
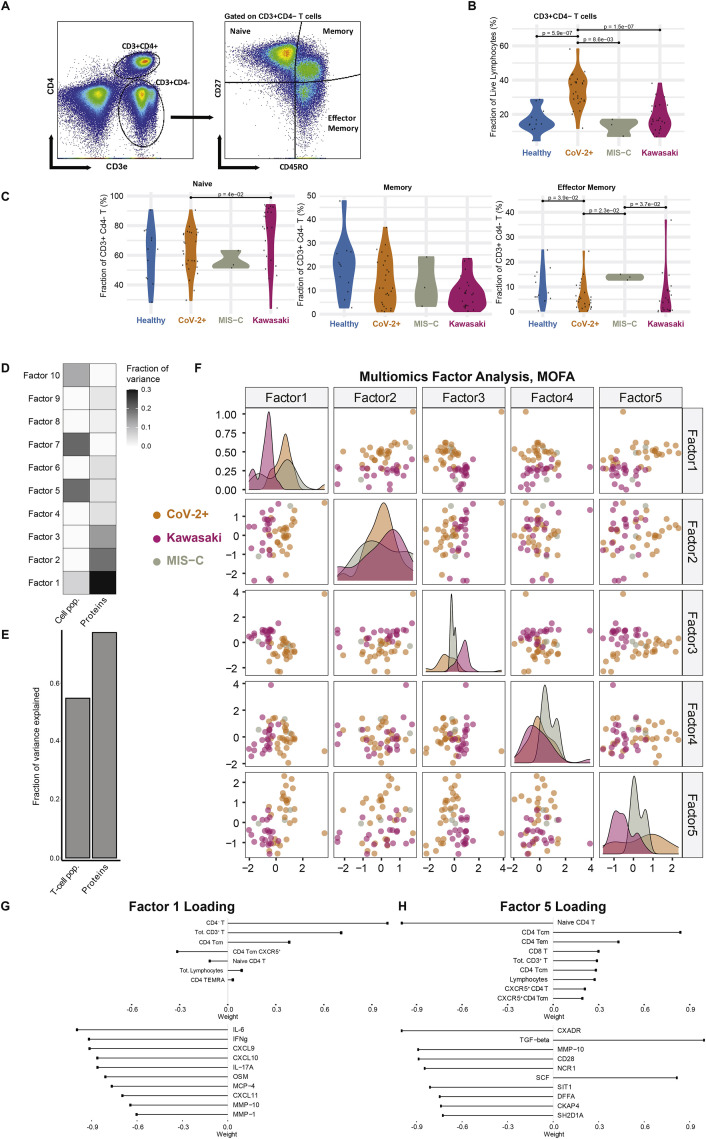
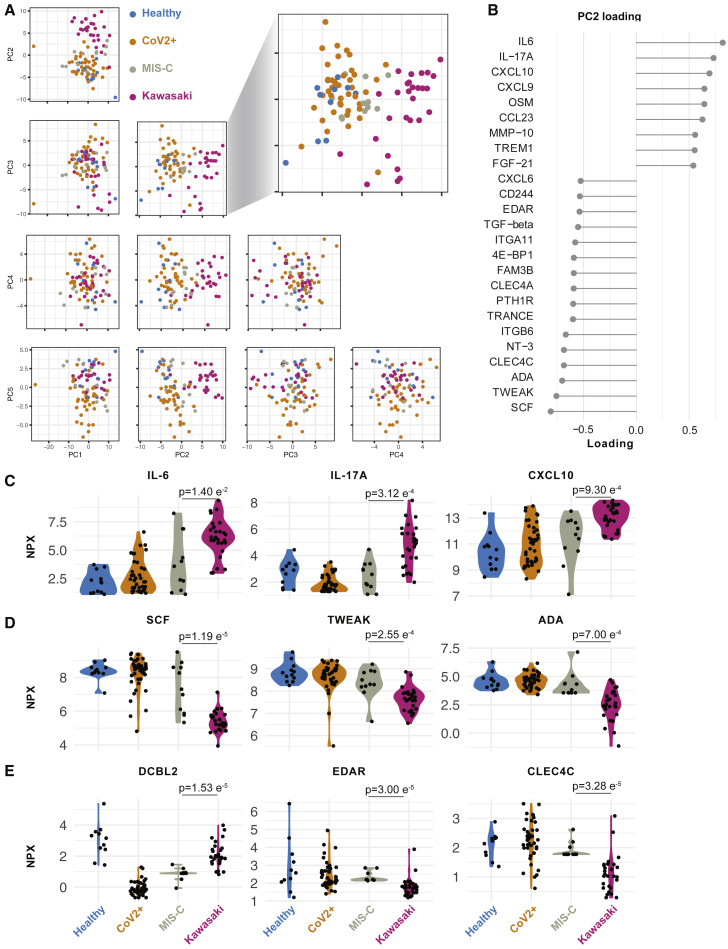
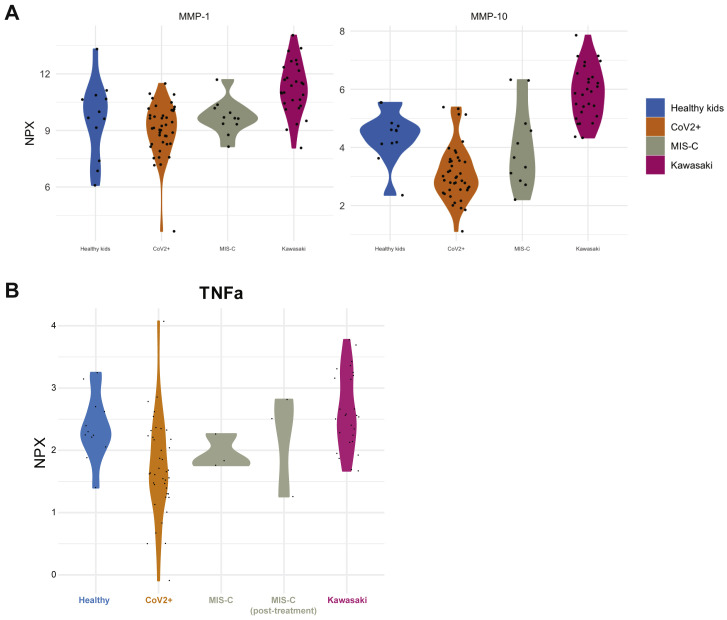
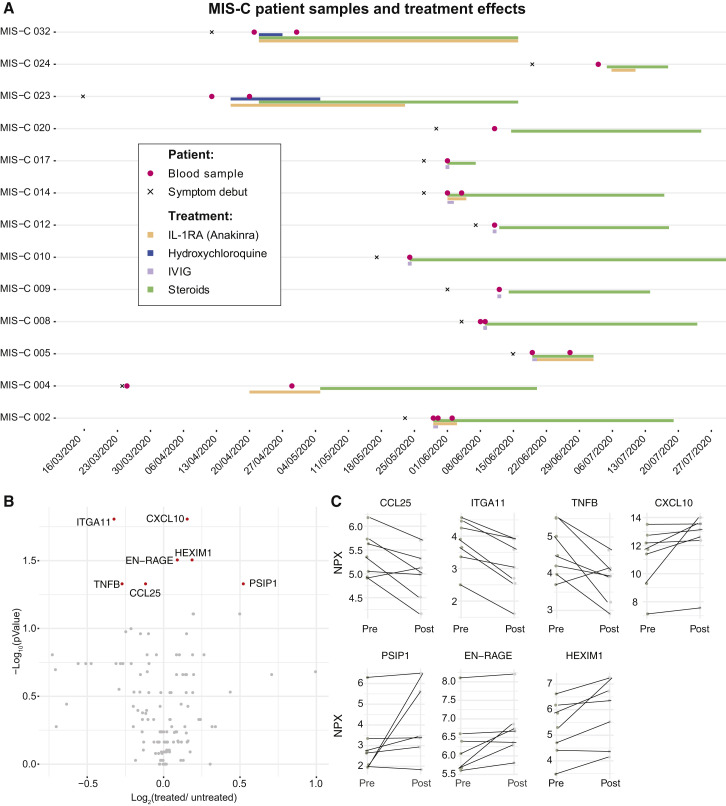
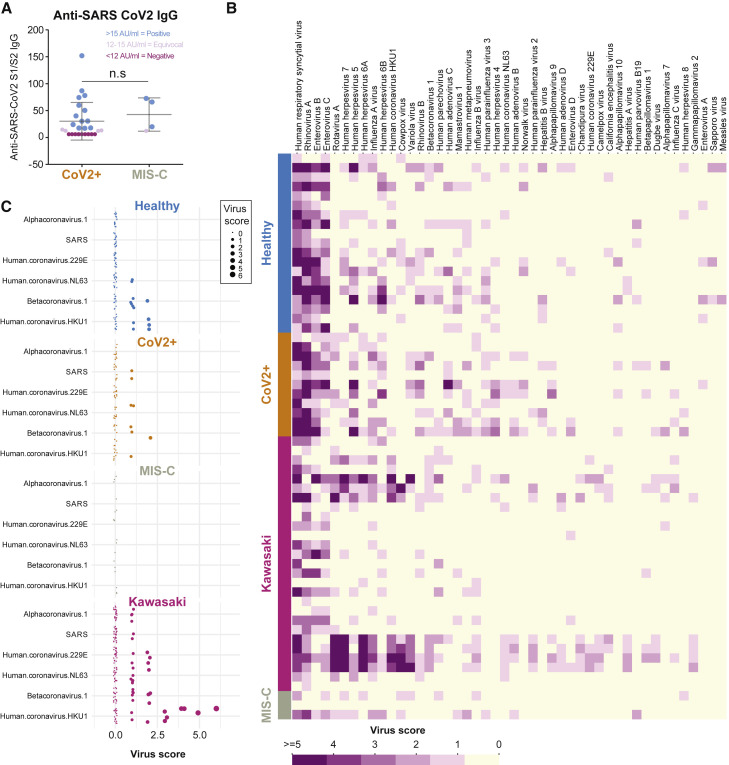
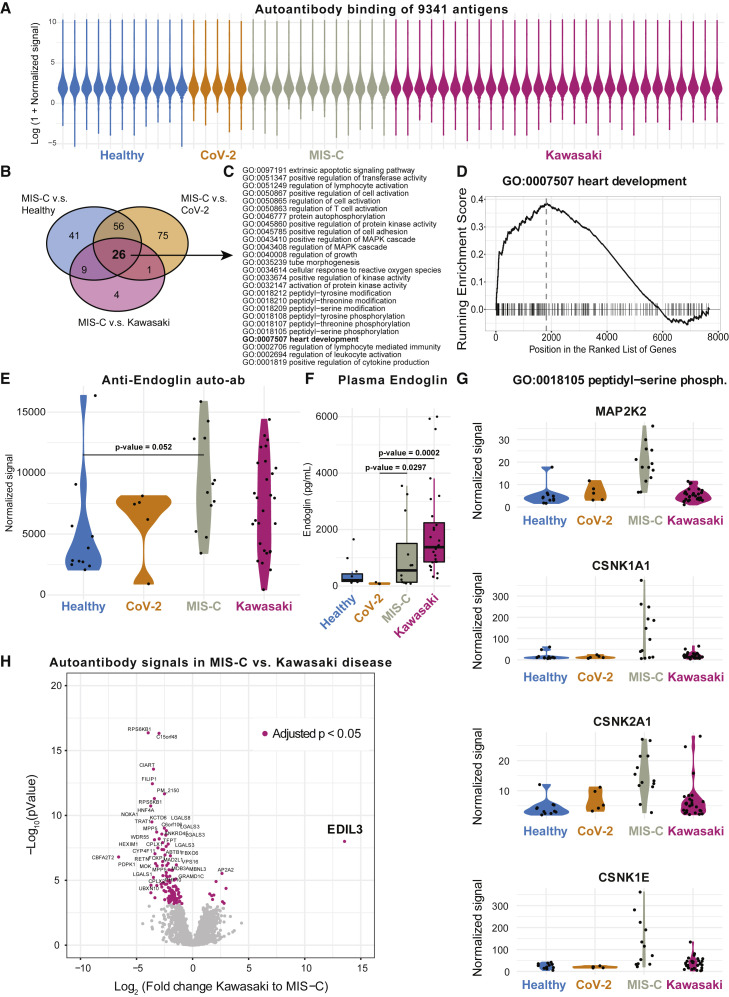
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection is typically very mild and often asymptomatic in children. A complication is the rare multisystem inflammatory syndrome in children (MIS-C) associated with COVID-19, presenting 4-6 weeks after infection as high fever, organ dysfunction, and strongly elevated markers of inflammation. The pathogenesis is unclear but has overlapping features with Kawasaki disease suggestive of vasculitis and a likely autoimmune etiology. We apply systems-level analyses of blood immune cells, cytokines, and autoantibodies in healthy children, children with Kawasaki disease enrolled prior to COVID-19, children infected with SARS-CoV-2, and children presenting with MIS-C. We find that the inflammatory response in MIS-C differs from the cytokine storm of severe acute COVID-19, shares several features with Kawasaki disease, but also differs from this condition with respect to T cell subsets, interleukin (IL)-17A, and biomarkers associated with arterial damage. Finally, autoantibody profiling suggests multiple autoantibodies that could be involved in the pathogenesis of MIS-C.
Keywords: COVID-19; IL-17A; Kawasaki disease; MIS-C; SARS-CoV-2; autoantibodies; hyperinflammation in children; multisystem inflammatory syndrome in children; systems immunology.
Copyright © 2020 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Interests P.B. and T.L. are founders and shareholders of Cytodelics AB (Stockholm, Sweden). P.B. is an advisor Scailyte AG (Switzerland).
Figures
Comment in
-
The Mystery of MIS-C Post-SARS-CoV-2 Infection.Trends Microbiol. 2020 Dec;28(12):956-958. doi: 10.1016/j.tim.2020.10.004. Epub 2020 Oct 14. Trends Microbiol. 2020. PMID: 33190685 Free PMC article.
References
-
- Anft M., Paniskaki K., Blazquez-Navarro A., Doevelaar A.A.N., Seibert F., Hoelzer B., Skrzypczyk S., Kohut E., Kurek J., Zapka J., et al. COVID-19 progression is potentially driven by T cell immunopathogenesis. medRxiv. 2020 doi: 10.1101/2020.04.28.20083089. - DOI
-
- Brodin P. Why is COVID-19 so mild in children? Acta Paediatr. 2020;109:1082–1083. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
