

Interim Analysis of a Phase 2 Open-Label Trial Assessing Burosumab Efficacy and Safety in Patients With Tumor-Induced Osteomalacia
- PMID: 32967046
- PMCID: PMC7988547
- DOI: 10.1002/jbmr.4184
Interim Analysis of a Phase 2 Open-Label Trial Assessing Burosumab Efficacy and Safety in Patients With Tumor-Induced Osteomalacia
Abstract
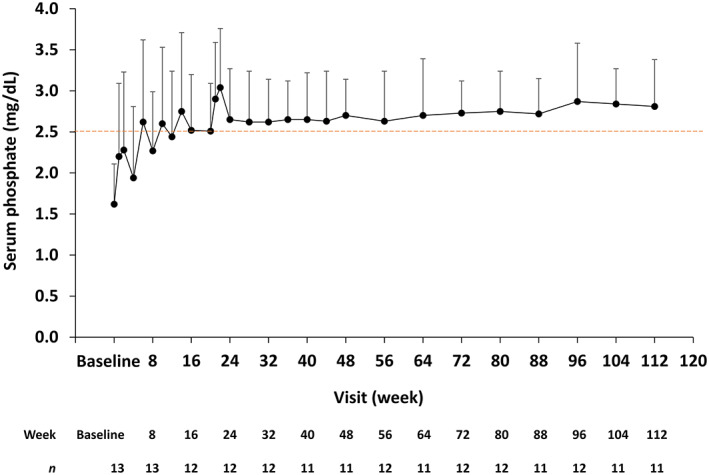
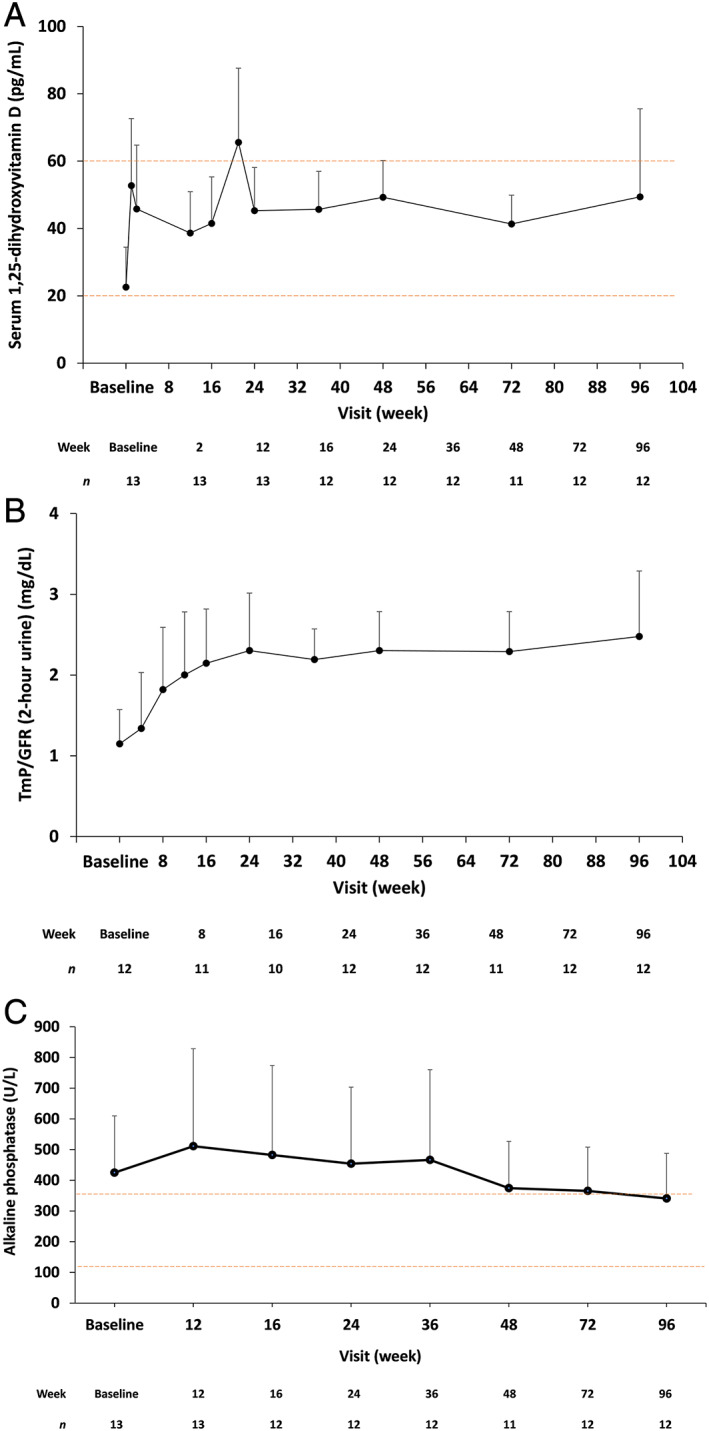
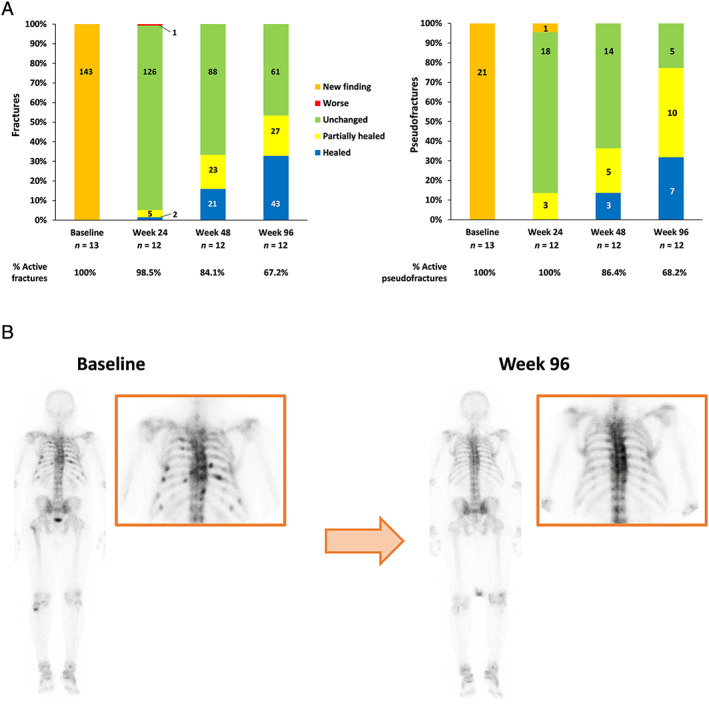
Patients with tumor-induced osteomalacia (TIO), an acquired paraneoplastic condition characterized by osteomalacia due to hypophosphatemia, exhibit a similar clinical picture to those with X-linked hypophosphatemic rickets/osteomalacia (XLH). The human monoclonal anti-fibroblast growth factor 23 (FGF23) antibody burosumab (KRN23) increases serum phosphate and improves bone turnover, fracture healing, pain, and physical function in XLH patients by inhibiting circulating FGF23; thus, burosumab is expected to be an effective treatment for TIO. We report here an interim analysis of a multicenter, open-label, intraindividual dose-adjustment study of burosumab (0.3 to 2.0 mg/kg every 4 weeks) in Japanese and Korean TIO patients. The primary endpoint was the fasting serum phosphate level at each visit. Key secondary endpoints were changes over time in bone biomarkers, pharmacodynamic markers, bone histomorphometric parameters, motor function, and patient-reported outcomes. Safety was assessed based on treatment-emergent adverse events (TEAEs). Thirteen patients received burosumab treatment, of whom 4 underwent bone biopsy. The mean dose after week 112 was approximately 1.0 mg/kg. After the first burosumab administration, mean serum phosphate levels increased and remained above the lower limit of normal and in the normal range from weeks 14 to 112. Bone biomarkers initially increased, reaching maximum values at week 16 or 24, and then gradually decreased. After burosumab treatment, patients were able to walk further (evaluated by the 6-minute walk test), reported decreased pain levels, and showed a tendency toward healing of baseline fractures and pseudofractures. Two patients discontinued, one each due to disease progression and consent withdrawal. Burosumab was generally well tolerated, with no treatment-related TEAEs of grade ≥3 and no treatment-related serious AEs. In conclusion, the interim results of this first study of burosumab to treat TIO patients indicate that this drug has the potential to provide clinical benefit for patients with unresectable tumors. The full study results are eagerly anticipated. © 2020 The Authors. Journal of Bone and Mineral Research published by Wiley Periodicals LLC on behalf of American Society for Bone and Mineral Research (ASBMR)..
Keywords: CLINICAL TRIALS; OSTEOMALACIA AND RICKETS; PTH/VIT D/FGF23.
© 2020 The Authors. Journal of Bone and Mineral Research published by Wiley Periodicals LLC on behalf of American Society for Bone and Mineral Research (ASBMR).
Figures
Comment in
-
Burosumab for Tumor-Induced Osteomalacia: Not Enough of a Good Thing.J Bone Miner Res. 2021 Dec;36(12):2453-2454. doi: 10.1002/jbmr.4318. Epub 2021 May 5. J Bone Miner Res. 2021. PMID: 33950530 No abstract available.
References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
