

Underwater versus conventional endoscopic mucosal resection for small size non-pedunculated colorectal polyps: a randomized controlled trial : (UEMR vs. CEMR for small size non-pedunculated colorectal polyps)
- PMID: 32967616
- PMCID: PMC7510164
- DOI: 10.1186/s12876-020-01457-y
Underwater versus conventional endoscopic mucosal resection for small size non-pedunculated colorectal polyps: a randomized controlled trial : (UEMR vs. CEMR for small size non-pedunculated colorectal polyps)
Abstract
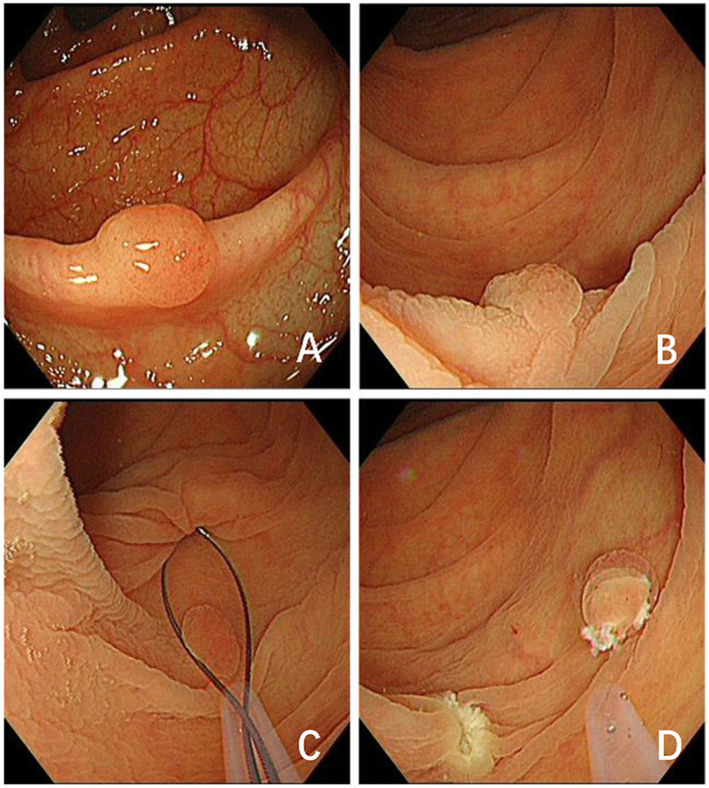
Background: Underwater endoscopic mucosal resection (UEMR) is a recently developed technique and can be performed during water-aided or ordinary colonoscopy for the treatment of colorectal polyps. The objective of this clinical trial was to evaluate the efficacy and safety of UEMR in comparison with conventional endoscopic mucosal resection (CEMR) of small non-pedunculated colorectal polyps.
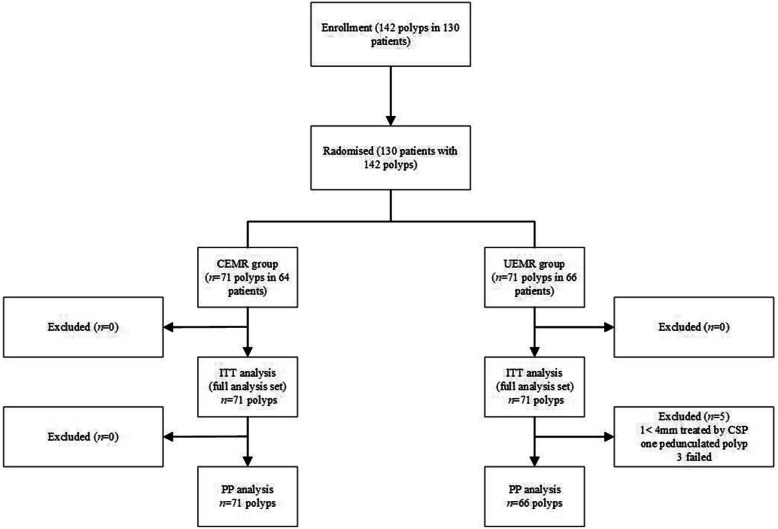
Methods: Patients with small size, non-pedunculated colorectal polyps (4-9 mm in size) who underwent colonoscopic polypectomy were enrolled in this multicenter randomized controlled clinical trial. The patients were randomly allocated to two groups, an UEMR group and a CEMR group. Efficacy and safety were compared between groups.
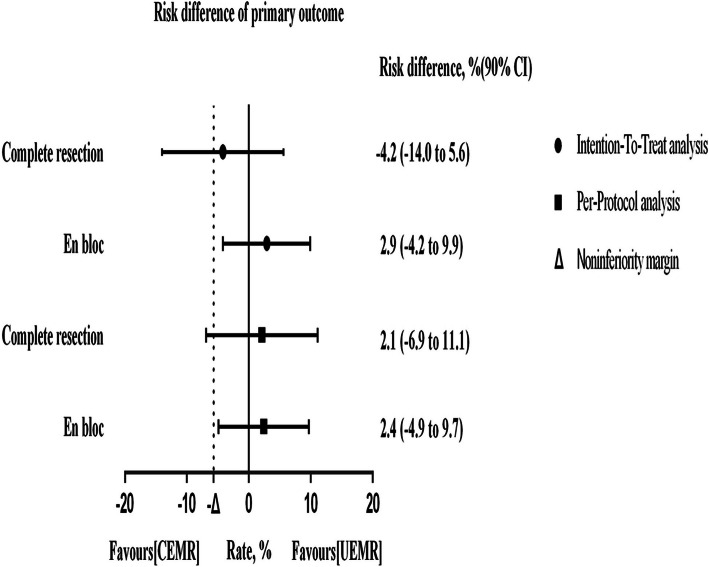
Results: In the intention-to-treat (ITT) analysis, the complete resection rate was 83.1% (59/71) in the UEMR group and 87.3% (62/71) in the CEMR group. The en-bloc resection rate was 94.4% (67/71) in the UEMR group and 91.5% (65/71) in the CEMR group (difference 2.9%; 90% CI - 4.2 to 9.9%), showed noninferiority (noninferiority margin - 5.7% < - 4.2%). No significant difference in procedure time (81 s vs. 72 s, P = 0.183) was observed. Early bleeding was observed in 1.4% of patients in the CEMR group (1/71) and 1.4% of patients in the UEMR group (1/71). None of the patients in the UEMR group complained of postprocedural bloody stool, whereas two patients in the CEMR group (2/64) reported this adverse event.
Conclusion: Our results indicate that UEMR is safer and just as effective as CEMR in En-bloc resection for the treatment of small colorectal polyps as such, UEMR is recommended as an alternative approach to excising small and non-pedunculated colorectal adenomatous polyps.
Trial registration: Clinical Trials.gov, NCT03833492 . Retrospectively registered on February 7, 2019.
Keywords: Colonic polyps; Colorectal cancer; Conventional endoscopic mucosal resection; Endoscopy; Underwater endoscopic mucosal resection.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Underwater endoscopic mucosal resection is superior to conventional endoscopic mucosal resection for medium-sized colorectal sessile polyps: a randomized controlled trial.Sci Rep. 2024 Dec 4;14(1):30172. doi: 10.1038/s41598-024-81817-w. Sci Rep. 2024. PMID: 39627535 Free PMC article. Clinical Trial.
-
Underwater vs Conventional Endoscopic Mucosal Resection of Large Sessile or Flat Colorectal Polyps: A Prospective Randomized Controlled Trial.Gastroenterology. 2021 Nov;161(5):1460-1474.e1. doi: 10.1053/j.gastro.2021.07.044. Epub 2021 Aug 8. Gastroenterology. 2021. PMID: 34371000 Clinical Trial.
-
Comparison of Underwater vs Conventional Endoscopic Mucosal Resection of Intermediate-Size Colorectal Polyps.Gastroenterology. 2019 Aug;157(2):451-461.e2. doi: 10.1053/j.gastro.2019.04.005. Epub 2019 Apr 11. Gastroenterology. 2019. PMID: 30981791 Clinical Trial.
-
Underwater versus conventional endoscopic mucosal resection for sessile colorectal polyps: an updated systematic review and meta-analysis.Rev Esp Enferm Dig. 2023 May;115(5):225-233. doi: 10.17235/reed.2022.8956/2022. Rev Esp Enferm Dig. 2023. PMID: 36148677
-
Underwater versus conventional endoscopic mucosal resection for colorectal lesions: a systematic review and meta-analysis of randomized clinical trials.Int J Colorectal Dis. 2023 Aug 8;38(1):208. doi: 10.1007/s00384-023-04505-7. Int J Colorectal Dis. 2023. PMID: 37552342
Cited by
-
Delayed Bleeding After Endoscopic Resection of Colorectal Polyps: Identifying High-Risk Patients.Clin Exp Gastroenterol. 2021 Dec 24;14:477-492. doi: 10.2147/CEG.S282699. eCollection 2021. Clin Exp Gastroenterol. 2021. PMID: 34992406 Free PMC article. Review.
-
Underwater endoscopic mucosal resection for colorectal lesions: Can it be an "Underwater" revolution?DEN Open. 2022 Jan 9;2(1):e84. doi: 10.1002/deo2.84. eCollection 2022 Apr. DEN Open. 2022. PMID: 35310727 Free PMC article. Review.
-
Underwater endoscopic mucosal resection is superior to conventional endoscopic mucosal resection for medium-sized colorectal sessile polyps: a randomized controlled trial.Sci Rep. 2024 Dec 4;14(1):30172. doi: 10.1038/s41598-024-81817-w. Sci Rep. 2024. PMID: 39627535 Free PMC article. Clinical Trial.
-
Algorithmic approach for endoscopic management of colorectal polyps: an up-to-date review.Gastroenterol Hepatol Bed Bench. 2025;18(1):39-52. doi: 10.22037/ghfbb.v18i1.3085. Gastroenterol Hepatol Bed Bench. 2025. PMID: 40734813 Free PMC article. Review.
-
Approaches and considerations in the endoscopic treatment of T1 colorectal cancer.Korean J Intern Med. 2024 Jul;39(4):563-576. doi: 10.3904/kjim.2023.487. Epub 2024 May 14. Korean J Intern Med. 2024. PMID: 38742279 Free PMC article. Review.
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. - PubMed
-
- Janout V, Kollárová H. Epidemiology of colorectal cancer. Biomed Pap Med Fac Univ Palacky, Olomouc, Czechoslovakia. 2001;145(1):5–10. - PubMed
-
- Zarchy T. Risk of submucosal saline injection for colonic polypectomy. Gastrointest Endosc. 1997;46(1):89–90. - PubMed
-
- Efthymiou M, Taylor AC, Desmond PV, Allen PB, Chen RY. Biopsy forceps is inadequate for the resection of diminutive polyps. Endoscopy. 2011;43(4):312–316. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
