

Tobacco exposure as a major modifier of oncologic outcomes in human papillomavirus (HPV) associated oropharyngeal squamous cell carcinoma
- PMID: 32967643
- PMCID: PMC7513300
- DOI: 10.1186/s12885-020-07427-7
Tobacco exposure as a major modifier of oncologic outcomes in human papillomavirus (HPV) associated oropharyngeal squamous cell carcinoma
Abstract
Background: The incidence of oropharyngeal squamous cell carcinoma (OPSCC) in the US is rapidly increasing, driven largely by the epidemic of human papillomavirus (HPV)-mediated OPSCC. Although survival for patients with HPV mediated OPSCC (HPV+ OPSCC) is generally better than that of patients with non-virally mediated OPSCC, this effect is not uniform. We hypothesized that tobacco exposure remains a critical modifier of survival for HPV+ OPSCC patients.
Methods: We conducted a retrospective analysis of 611 OPSCC patients with concordant p16 and HPV testing treated at a single institute (2002-2013). Survival analysis was performed using Kaplan-Meier analysis and Cox regression. Recursive partitioning analysis (RPA) was used to define tobacco exposure associated with survival (p < 0.05).
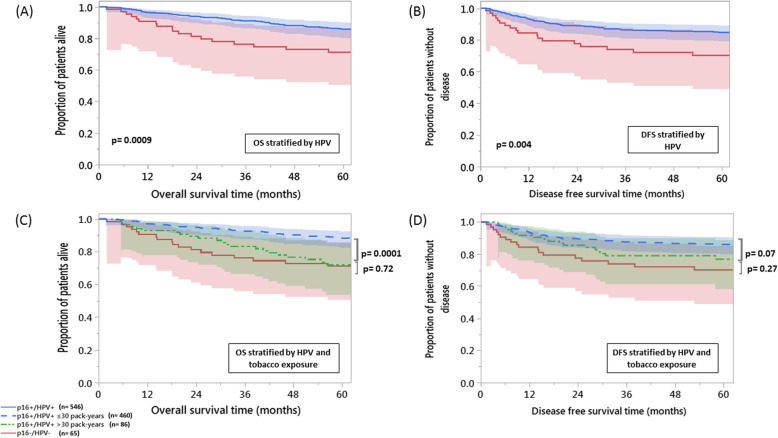
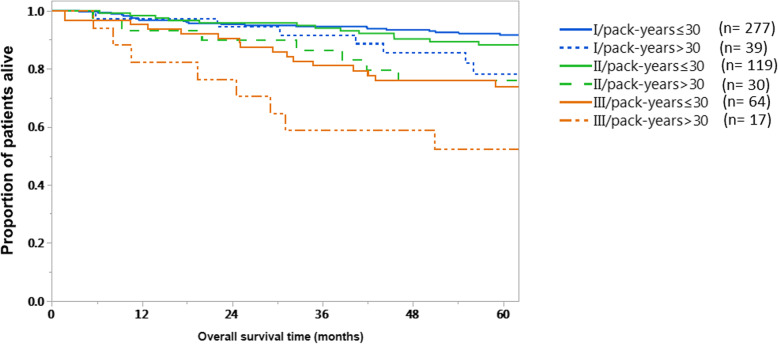
Results: Tobacco exposure impacted overall survival (OS) for HPV+ patients on univariate and multivariate analysis (p = 0.002, p = 0.003 respectively). RPA identified 30 pack-years (PY) as a threshold at which survival became significantly worse in HPV+ patients. OS and disease-free survival (DFS) for HPV+ > 30 PY patients didn't differ significantly from HPV- patients (p = 0.72, p = 0.27, respectively). HPV+ > 30 PY patients had substantially lower 5-year OS when compared to their ≤30 PYs counterparts: 78.4% vs 91.6%; p = 0.03, 76% vs 88.3%; p = 0.07, and 52.3% vs 74%; p = 0.05, for stages I, II, and III (AJCC 8th Edition Manual), respectively.
Conclusions: Tobacco exposure can eliminate the survival benefit associated with HPV+ status in OPSCC patients. Until this effect can be clearly quantified using prospective datasets, de-escalation of treatment for HPV + OPSCC smokers should be avoided.
Keywords: Human papillomavirus; Oropharyngeal carcinoma; Radiotherapy; Tobacco.
Conflict of interest statement
The authors have no competing interests to report.
Figures
References
-
- Gillison ML, Koch WM, Capone RB, et al. Evidence for a causal association between human papillomavirus and a subset of head and neck cancers. J Natl Cancer Inst. 2000;92:709–720. - PubMed
-
- Cohen MA, Weinstein GS, O'Malley BW, Jr, Feldman M, Quon H. Transoral robotic surgery and human papillomavirus status: oncologic results. Head Neck. 2011;33:573–580. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
