

Mycobacterium haemophilum scleritis: two case reports and review of literature
- PMID: 32967654
- PMCID: PMC7513486
- DOI: 10.1186/s12886-020-01649-w
Mycobacterium haemophilum scleritis: two case reports and review of literature
Abstract
Background: Mycobacterium haemophilum is a rare and emerging nontuberculous mycobacteria (NTM). It normally causes localized or disseminated systemic diseases, particularly skin infections and arthritis in severely immunocompromised patients. There have been 5 cases of M. haemophilum ocular infections reported in the literature. Only 1 case presented with scleritis with keratitis. Here, we reported 2 cases of M. haemophilum scleritis. One of them was immunocompetent host and had keratitis with radial keratoneuritis as a presenting sign.
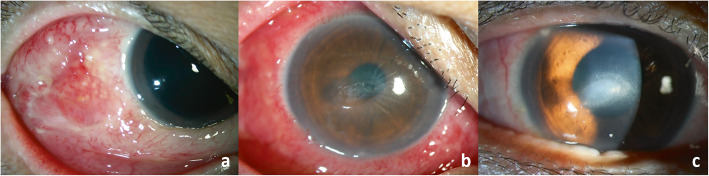
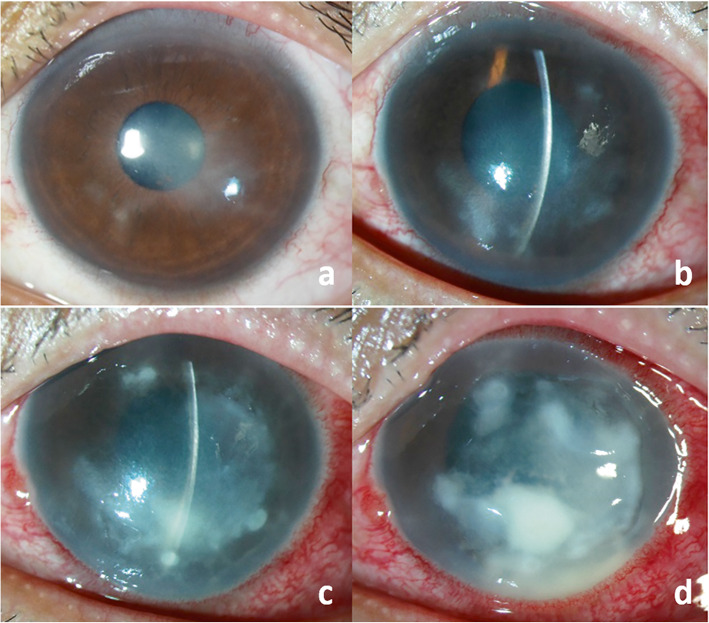
Case presentation: Case 1: A 52-year-old Thai female with rheumatoid arthritis presented with scleritis. Conjunctival scraping was carried out and the culture result was positive for M. haemophilum. Despite receiving systemic and topical antibiotics, her clinical symptoms and signs worsened. Surgical debridement was performed. After surgery, the lesion was significantly improved and finally turned to conjunctival scarring. Case 2: A 32-year old healthy Thai male without underlying disease presented with nodular scleritis and keratouveitis with multiple radial keratoneuritis. Surgical debridement of the scleral nodule was performed. Initial microbiological investigations were negative. Herpes ocular infections was suspected. Topical antibiotics, oral acyclovir, low-dose topical steroids and systemic steroids were started. The scleral inflammation subsided but later the keratitis relapsed, requiring corneal biopsy. Histopathology of the specimen revealed acid-fast bacteria and M. haemophilum was identified by polymerase chain reaction (PCR) and sequencing. The diagnosis of Mycobacterial keratitis was made. Although using the combination of systemic and topical antibiotics, his clinical status progressively deteriorated. Multiple therapeutic penetrating keratoplasties were required to eradicate the infection. No recurrence was found during the 1-year follow-up in both cases.
Conclusions: M. haemophilum can cause scleritis and keratitis, even in immunocompenent host. Radial keraoneuritis is first described in M. haemophilum keratitis. NTM keratitis should be considered in the differential diagnosis of patients with radial keratoneuritis. Increased awareness and early diagnosis using appropriate culture conditions and molecular techniques are important for the proper treatment of this infection. Prompt surgical intervention appears to be vital for successful management of M. haemophilum scleritis and keratitis.
Keywords: Case report; Keratitis; Mycobacterium haemophilum; Nontuberculous mycobacteria; Radial keratoneuritis; Scleritis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Mycobacterium haemophilum necrotising keratitis in a cornea with no prior surgical intervention.BMJ Case Rep. 2025 Apr 8;18(4):e260340. doi: 10.1136/bcr-2024-260340. BMJ Case Rep. 2025. PMID: 40199603 Free PMC article.
-
Ocular Mycobacterium haemophilum infection originating in the cornea: a case report.BMC Infect Dis. 2023 Mar 7;23(1):140. doi: 10.1186/s12879-023-08094-2. BMC Infect Dis. 2023. PMID: 36882753 Free PMC article.
-
Clinicopathologic case report: scleral buckle associated nontuberculous mycobacterial scleritis.Semin Ophthalmol. 2004 Sep-Dec;19(3-4):101-4. doi: 10.1080/08820530490882517. Semin Ophthalmol. 2004. PMID: 15590546
-
Clinical manifestations, diagnosis, and treatment of Mycobacterium haemophilum infections.Clin Microbiol Rev. 2011 Oct;24(4):701-17. doi: 10.1128/CMR.00020-11. Clin Microbiol Rev. 2011. PMID: 21976605 Free PMC article. Review.
-
Nontuberculous mycobacterial ocular and adnexal infections.Surv Ophthalmol. 2012 May-Jun;57(3):202-35. doi: 10.1016/j.survophthal.2011.10.006. Surv Ophthalmol. 2012. PMID: 22516536 Review.
Cited by
-
Disseminated cutaneous Mycobacterium haemophilum infection in a patient on infliximab for rheumatoid arthritis.BMJ Case Rep. 2022 Jan 17;15(1):e245853. doi: 10.1136/bcr-2021-245853. BMJ Case Rep. 2022. PMID: 35039354 Free PMC article.
-
Orbital and conjunctival nontuberculous mycobacteria infection.Taiwan J Ophthalmol. 2022 Aug 25;13(3):393-397. doi: 10.4103/2211-5056.354534. eCollection 2023 Jul-Sep. Taiwan J Ophthalmol. 2022. PMID: 38089514 Free PMC article.
-
Mycobacterium haemophilum necrotising keratitis in a cornea with no prior surgical intervention.BMJ Case Rep. 2025 Apr 8;18(4):e260340. doi: 10.1136/bcr-2024-260340. BMJ Case Rep. 2025. PMID: 40199603 Free PMC article.
-
Ocular infections associated with atypical mycobacteria: A review.Indian J Ophthalmol. 2024 Jan 1;72(1):19-28. doi: 10.4103/IJO.IJO_560_23. Epub 2023 Dec 22. Indian J Ophthalmol. 2024. PMID: 38131566 Free PMC article. Review.
-
Ocular Mycobacterium haemophilum infection originating in the cornea: a case report.BMC Infect Dis. 2023 Mar 7;23(1):140. doi: 10.1186/s12879-023-08094-2. BMC Infect Dis. 2023. PMID: 36882753 Free PMC article.
References
-
- van Ingen J, Boeree MJ, Dekhuijzen PN, van Soolingen D. Environmental sources of rapid growing nontuberculous mycobacteria causing disease in humans. Clin Microbiol Infect. 2009;15:888–893. - PubMed
-
- Moorthy RS, Valluri S, Rao NA. Nontuberculous mycobacterial ocular and adnexal infections. Surv Ophthalmol. 2012;57:202–235. - PubMed
-
- Modi D, Pyatetsky D, Edward DP, Ulanski LJ, Pursell KJ, Tessler HH, et al. Mycobacterium haemophilum: a rare cause of endophthalmitis. Retina. 2007;27:1148–1151. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
