

PET/MRI of atherosclerosis
- PMID: 32968664
- PMCID: PMC7487378
- DOI: 10.21037/cdt.2020.02.09
PET/MRI of atherosclerosis
Abstract
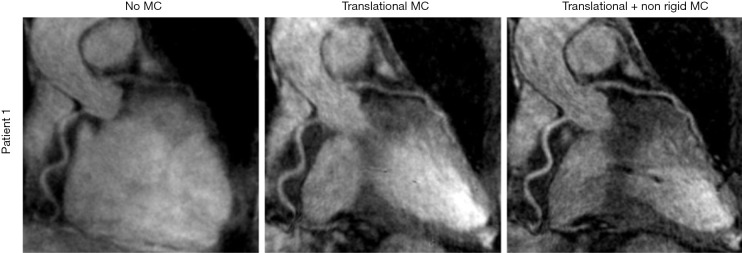
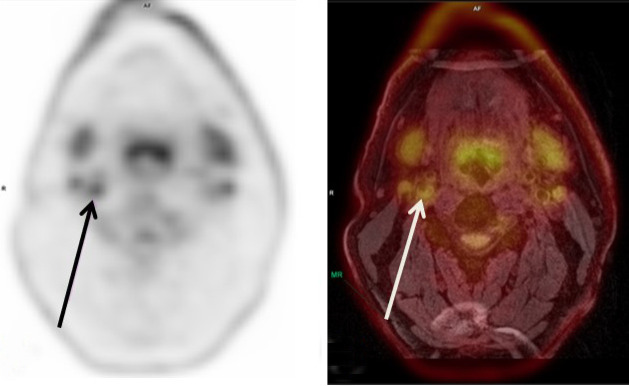
Myocardial infarction and stroke are the most prevalent global causes of death. Each year 15 million people worldwide die due to myocardial infarction or stroke. Rupture of a vulnerable atherosclerotic plaque is the main underlying cause of stroke and myocardial infarction. Key features of a vulnerable plaque are inflammation, a large lipid-rich necrotic core (LRNC) with a thin or ruptured overlying fibrous cap, and intraplaque hemorrhage (IPH). Noninvasive imaging of these features could have a role in risk stratification of myocardial infarction and stroke and can potentially be utilized for treatment guidance and monitoring. The recent development of hybrid PET/MRI combining the superior soft tissue contrast of MRI with the opportunity to visualize specific plaque features using various radioactive tracers, paves the way for comprehensive plaque imaging. In this review, the use of hybrid PET/MRI for atherosclerotic plaque imaging in carotid and coronary arteries is discussed. The pros and cons of different hybrid PET/MRI systems are reviewed. The challenges in the development of PET/MRI and potential solutions are described. An overview of PET and MRI acquisition techniques for imaging of atherosclerosis including motion correction is provided, followed by a summary of vessel wall imaging PET/MRI studies in patients with carotid and coronary artery disease. Finally, the future of imaging of atherosclerosis with PET/MRI is discussed.
Keywords: Atherosclerosis; PET/MRI; hybrid imaging; vascular; vulnerable plaque.
2020 Cardiovascular Diagnosis and Therapy. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/cdt.2020.02.09). The series “Advanced Imaging in The Diagnosis of Cardiovascular Diseases” was commissioned by the editorial office without any funding or sponsorship. Dr. RPMM reports grants from Stichting de Weijerhorst, outside the submitted work; Prof. Dr. MEK reports grants from European Union’s Horizon 2020 research and innovation program under the Marie Skłodowska-Curie grant agreement No. 722609 and a grant from NWO/ASPASIA, during the conduct of the study; grant from Stichting De Weijerhorst, grant from NWO Hestia, outside the submitted work. The other authors have no conflicts of interest to declare.
Figures



References
-
- World Health Organization. Cardiovascular diseases (CVDs). 2017. Available online: http://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-.... Accessed 4 Sep 2019.
-
- Benjamin EJ BM, Chiuve SE, Cushman M, et al. Heart Disease and Stroke Statistics 2017 At a Glance. 2017.
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous