

Pathological features of COVID-19-associated myocardial injury: a multicentre cardiovascular pathology study
- PMID: 32968776
- PMCID: PMC7543528
- DOI: 10.1093/eurheartj/ehaa664
Pathological features of COVID-19-associated myocardial injury: a multicentre cardiovascular pathology study
Abstract
Aims: Coronavirus disease 2019 (COVID-19) due to severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) has been associated with cardiovascular features of myocardial involvement including elevated serum troponin levels and acute heart failure with reduced ejection fraction. The cardiac pathological changes in these patients with COVID-19 have yet to be well described.
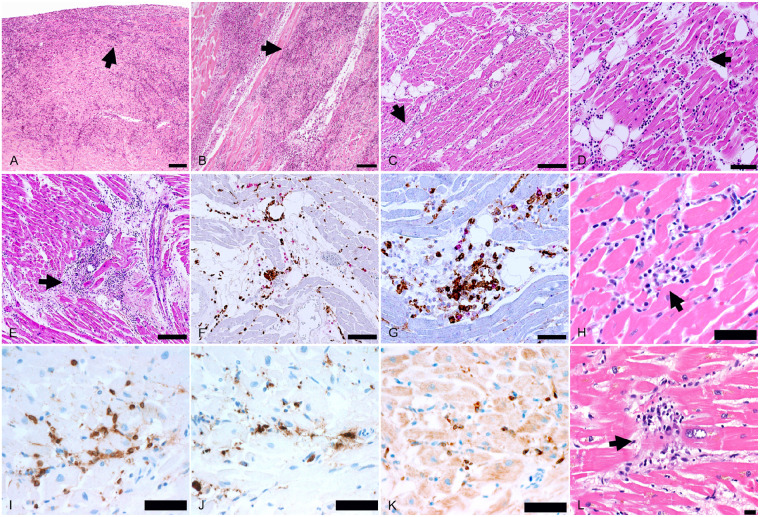
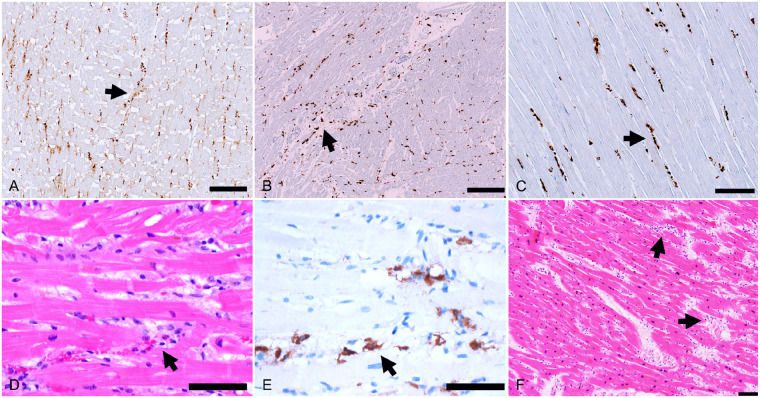
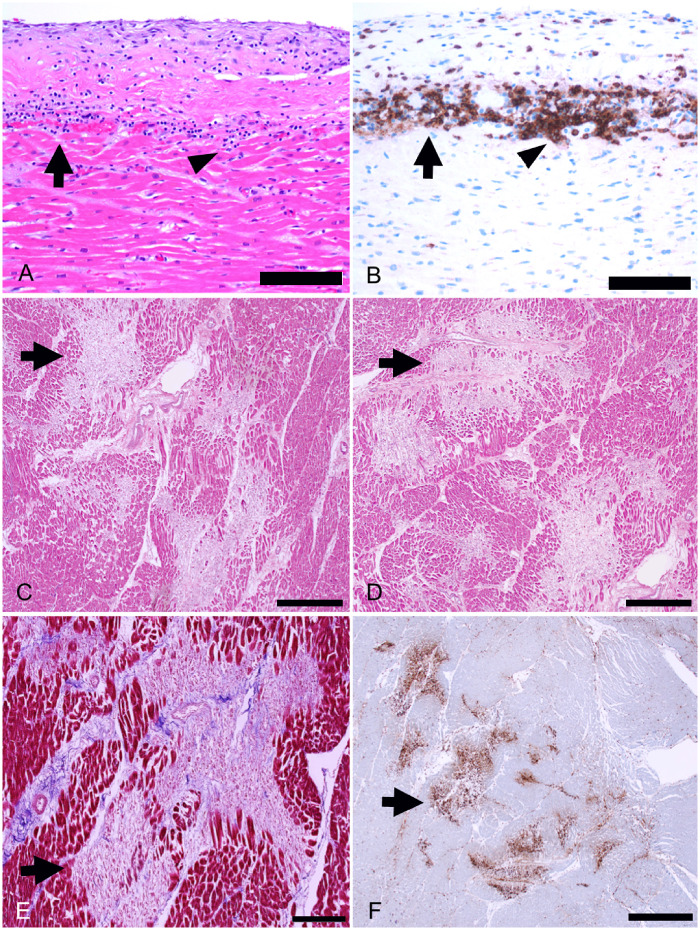
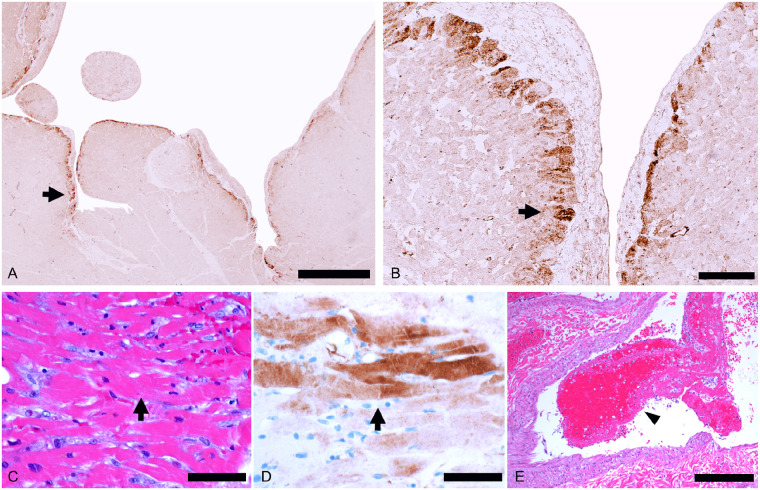
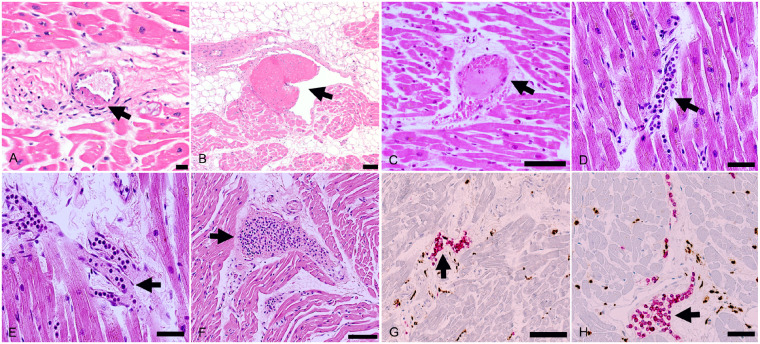
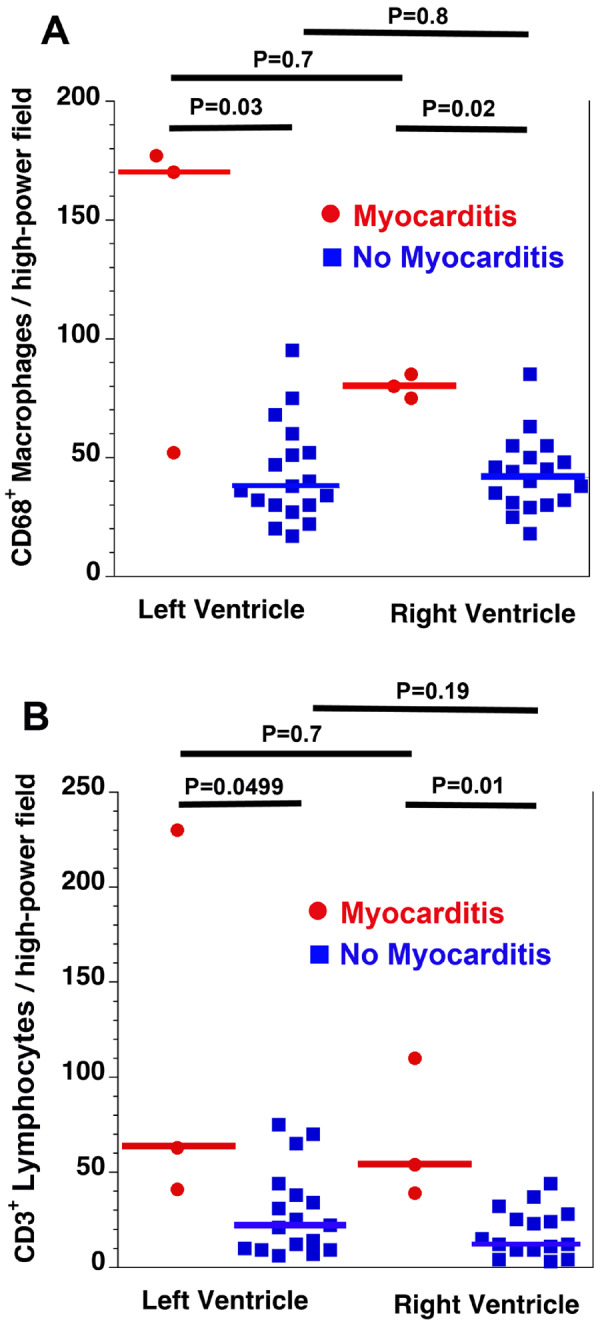
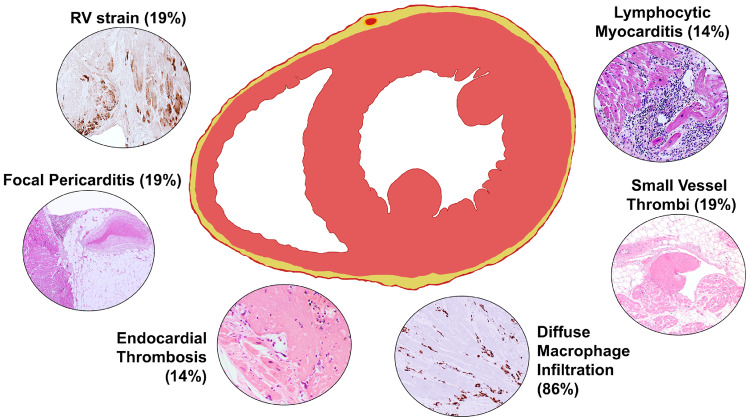
Methods and results: In an international multicentre study, cardiac tissue from the autopsies of 21 consecutive COVID-19 patients was assessed by cardiovascular pathologists. The presence of myocarditis, as defined by the presence of multiple foci of inflammation with associated myocyte injury, was determined, and the inflammatory cell composition analysed by immunohistochemistry. Other forms of acute myocyte injury and inflammation were also described, as well as coronary artery, endocardium, and pericardium involvement. Lymphocytic myocarditis was present in 3 (14%) of the cases. In two of these cases, the T lymphocytes were CD4 predominant and in one case the T lymphocytes were CD8 predominant. Increased interstitial macrophage infiltration was present in 18 (86%) of the cases. A mild pericarditis was present in four cases. Acute myocyte injury in the right ventricle, most probably due to strain/overload, was present in four cases. There was a non-significant trend toward higher serum troponin levels in the patients with myocarditis compared with those without myocarditis. Disrupted coronary artery plaques, coronary artery aneurysms, and large pulmonary emboli were not identified.
Conclusions: In SARS-CoV-2 there are increased interstitial macrophages in a majority of the cases and multifocal lymphocytic myocarditis in a small fraction of the cases. Other forms of myocardial injury are also present in these patients. The macrophage infiltration may reflect underlying diseases rather than COVID-19.
Keywords: Autopsy; COVID-19; Heart; Macrophages; Myocarditis; Myocardium; SARS; SARS-CoV-2.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2020. For permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
The significance of COVID-19-associated myocardial injury: how overinterpretation of scientific findings can fuel media sensationalism and spread misinformation.Eur Heart J. 2020 Oct 14;41(39):3836-3838. doi: 10.1093/eurheartj/ehaa727. Eur Heart J. 2020. PMID: 33006608 Free PMC article. No abstract available.
References
-
- Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, Xiang J, Wang Y, Song B, Gu X, Guan L, Wei Y, Li H, Wu H, Xu J, Tu S, Zhang Y, Chen H, Cao B. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet 2020;395:1054–1062. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
