

Comparison of hyperspectral imaging and fluorescence angiography for the determination of the transection margin in colorectal resections-a comparative study
- PMID: 32968892
- PMCID: PMC7801293
- DOI: 10.1007/s00384-020-03755-z
Comparison of hyperspectral imaging and fluorescence angiography for the determination of the transection margin in colorectal resections-a comparative study
Erratum in
-
Correction to: Comparison of hyperspectral imaging and fluorescence angiography for the determination of the transection margin in colorectal resections-a comparative study.Int J Colorectal Dis. 2022 Aug;37(8):1921. doi: 10.1007/s00384-022-04227-2. Int J Colorectal Dis. 2022. PMID: 35916906 Free PMC article. No abstract available.
Abstract
Purpose: One relevant aspect for anastomotic leakage in colorectal surgery is blood perfusion of both ends of the anastomosis. The clinical evaluation of this issue is limited, but new methods like fluorescence angiography with indocyanine green or non-invasive and contactless hyperspectral imaging have evolved as objective parameters for perfusion evaluation.
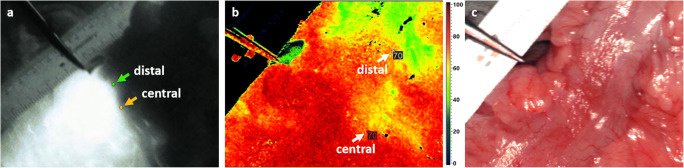
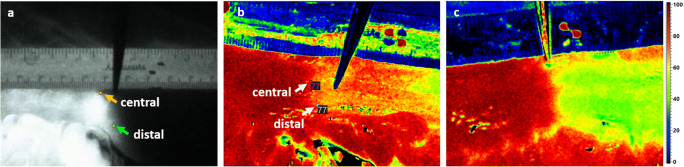
Methods: In this prospective, non-randomized, open-label and two-arm study, fluorescence angiography and hyperspectral imaging were compared in 32 consecutive patients with each other and with the clinical assessment by the surgeon. After preparation of the bowel and determination of the surgical resection line, the tissue was evaluated with hyperspectral imaging for 5 min before and after cutting the marginal artery and assessed by 6 hyperspectral pictures followed by fluorescence angiography with indocyanine green.
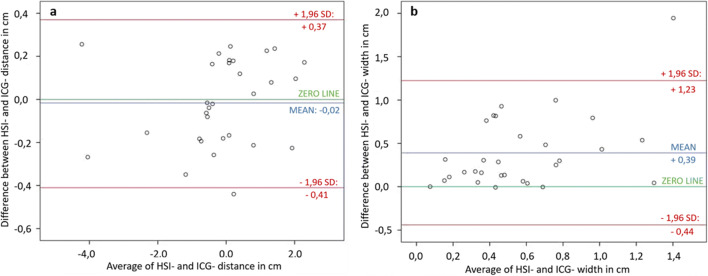
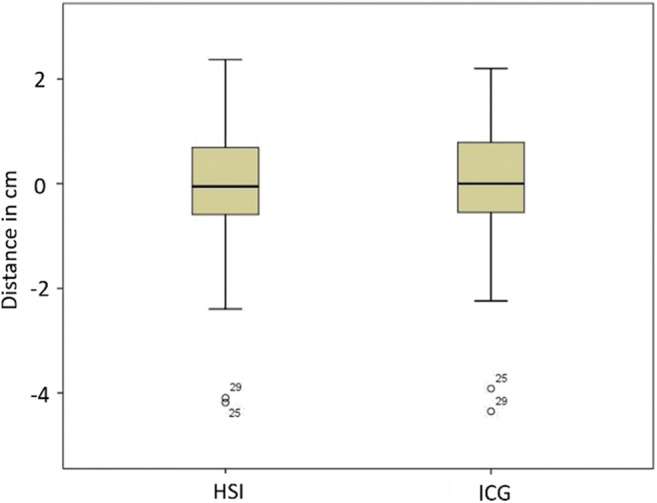
Results: In 30 of 32 patients, the image data could be evaluated and compared. Both methods provided a comparable borderline between well-perfused and poorly perfused tissue (p = 0.704). In 15 cases, the surgical resection line was shifted to the central position due to the imaging. The border zone was sharper in fluorescence angiography and best assessed 31 s after injection. With hyperspectral imaging, the border zone was visualized wider and with more differences between proximal and distal border.
Conclusion: Hyperspectral imaging and fluorescence angiography provide similar results in determining the perfusion border. Both methods allow a good and safe visualization of the blood perfusion at the central resection margin to create a well-perfused anastomosis.
Trial registration: This study was registered at Clinicaltrials.gov ( NCT04226781 ) on January 13, 2020.
Keywords: Anastomotic leak; Colorectal resection; Fluorescence angiography (FA); Hyperspectral imaging (HSI); Indocyanine green (ICG).
Conflict of interest statement
Hannes Köhler is an Employee of Diaspective GmbH. The authors declare that they have no conflict of interest.
Figures
References
-
- Phillips B (2016) Reducing gastrointestinal anastomotic leak rates: review of challenges and solutions. OAS 5. 10.2147/OAS.S54936
-
- Dana A, Telem MD, Edward H, Chin MD, Scott Q, Nguyen MD et al (2010) Risk factors for anastomotic leak following colorectal surgery. Am Med Assoc:1–6 - PubMed
-
- Frasson M, Flor-Lorente B, Rodríguez JLR, Granero-Castro P, Hervás D, Alvarez Rico MA, Brao MJ, Sánchez González JM, Garcia-Granero E, ANACO Study Group Risk factors for anastomotic leak after colon resection for cancer: multivariate analysis and nomogram from a multicentric, prospective, national study with 3193 patients. Ann Surg. 2015;262(2):321–330. doi: 10.1097/SLA.0000000000000973. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
