

Corticosteroid and Local Anesthetic Use Trends for Large Joint and Bursa Injections: Results of a Survey of Sports Medicine Physicians
- PMID: 32969178
- PMCID: PMC8674102
- DOI: 10.1002/pmrj.12499
Corticosteroid and Local Anesthetic Use Trends for Large Joint and Bursa Injections: Results of a Survey of Sports Medicine Physicians
Abstract
Background: Physician decision-making surrounding choices for large joint and bursa injections is poorly defined, yet influences patient safety and treatment effectiveness.
Objective: To identify practice patterns and rationale related to injectate choices for large joint and bursal injections performed by physician members of the American Medical Society for Sports Medicine (AMSSM).
Design: An electronic survey was sent to 3400 members of the AMSSM. Demographic variables were collected: primary specialty (residency), training location, practice location, years of clinical experience, current practice type, and rationale for choosing an injectate.
Participants: A total of 674 physicians responded (minimum response rate of 20%).
Intervention: Not applicable.
Main outcome measures: Outcomes of interest included corticosteroid type and dose, local anesthetic type, and total injectate volume for each large joint or bursa (hip, knee, and shoulder).
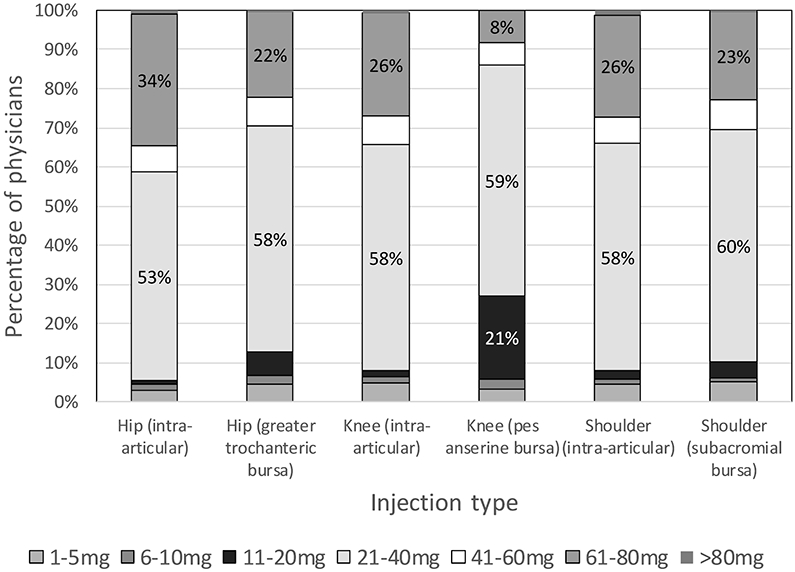
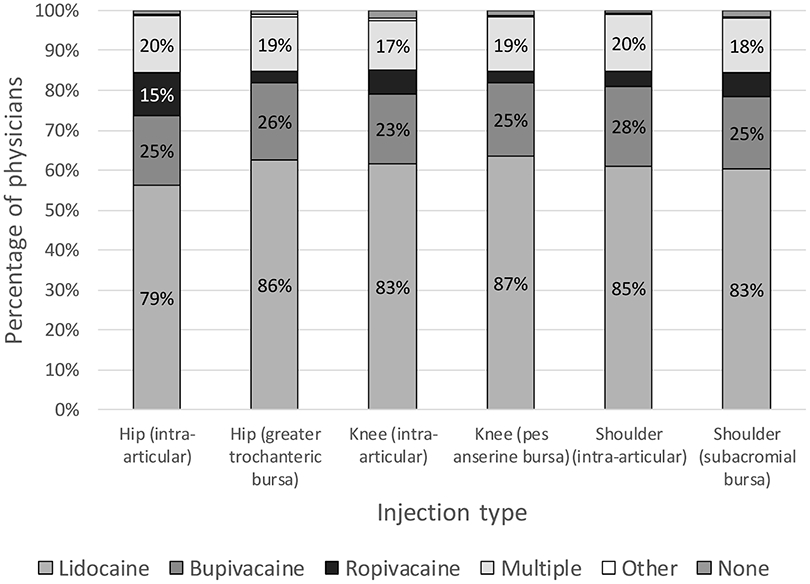
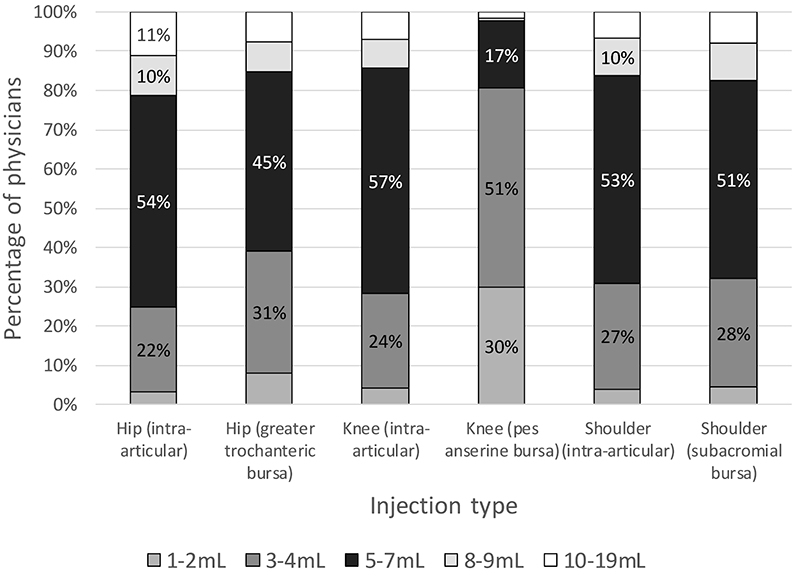
Results: Most respondents used triamcinolone (50% to 56% of physicians, depending on injection location) or methylprednisolone (25% to 29% of physicians), 21 to 40 mg (53% to 60% of physicians), diluted with lidocaine (79% to 87%) for all large joint or bursa injections. It was noted that 36.2% (244/674) of respondents reported using >40 mg for at least one injection type. Most (90.5%, 610/674) reported using an anesthetic other than ropivacaine for at least one type of joint or bursa injection. Physicians who reported lidocaine use were less likely to report that their injectate choice was based on the literature that they reviewed (odds ratio [OR] 0.41 [0.27-0.62], P < .001). Respondents predominantly used 5 to 7 mL of total injectate for all large joints or bursae (45% to 54% of respondents), except for the pes anserine bursa, where 3-4 mL was more common (51% of physicians).
Conclusions: It appears that triamcinolone and methylprednisolone are the most commonly used corticosteroids for sports medicine physicians; most physicians use 21 to 40 mg of corticosteroid for all injections, and lidocaine is the most-often used local anesthetic; very few use ropivacaine. Over one-third of respondents used high-dose (>40 mg triamcinolone or methylprednisolone) for at least one joint or bursa.
© 2020 American Academy of Physical Medicine and Rehabilitation.
Figures

References
-
- Miller JH, White J, Norton TH. The value of intra-articular injections in osteoarthritis of the knee. J Bone Jt Surg Br. 1958;40-b(4):636–643. http://www.bjj.boneandjoint.org.uk/content/jbjsbr/40-B/4/636.full.pdf. - PubMed
-
- Cushman DM, Bruno B, Christiansen J, Schultz A, McCormick ZL. Efficacy of Injected Corticosteroid Type, Dose, and Volume for Pain in Large Joints: A Narrative Review. PM R. 2018;10(7):748–757. http://www.ncbi.nlm.nih.gov/pubmed/29407227. - PubMed
-
- Skedros JG, Hunt KJ, Pitts TC. Variations in corticosteroid/anesthetic injections for painful shoulder conditions: comparisons among orthopaedic surgeons, rheumatologists, and physical medicine and primary-care physicians. BMC Musculoskelet Disord. 2007;8:63. http://www.ncbi.nlm.nih.gov/pubmed/17617900. - PMC - PubMed
-
- Deshmukh AJ, Panagopoulos G, Alizadeh A, Rodriguez JA, Klein DA. Intra-articular hip injection: does pain relief correlate with radiographic severity of osteoarthritis? Skelet Radiol. 2011;40(11):1449–1454. http://link.springer.com/article/10.1007%2Fs00256-011-1120-8. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
