

Predictors of Bleeding in the Perioperative Anticoagulant Use for Surgery Evaluation Study
- PMID: 32969288
- PMCID: PMC7792425
- DOI: 10.1161/JAHA.120.017316
Predictors of Bleeding in the Perioperative Anticoagulant Use for Surgery Evaluation Study
Abstract
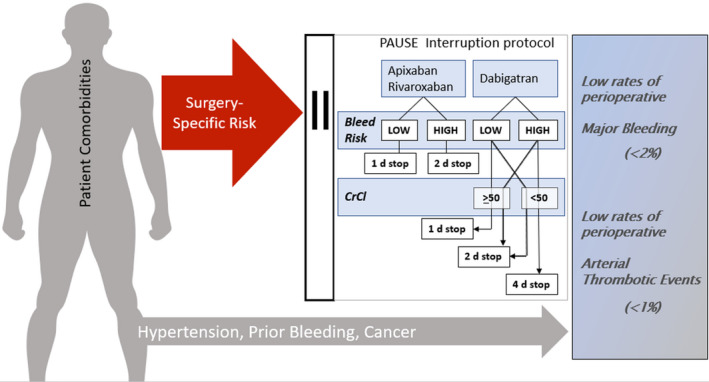
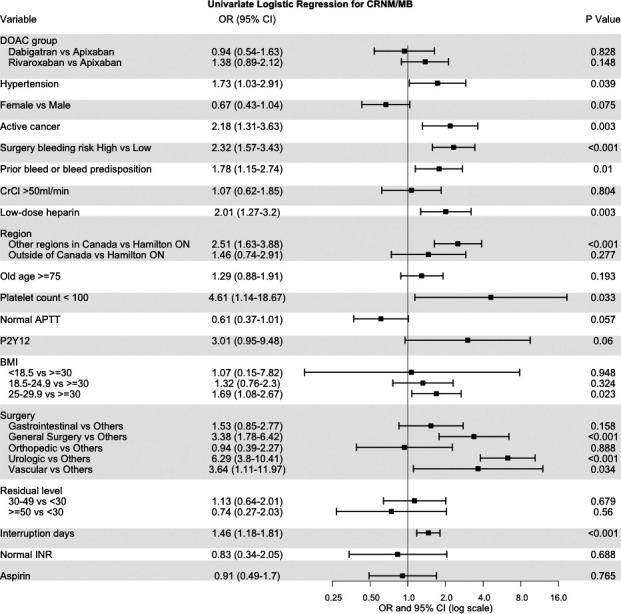
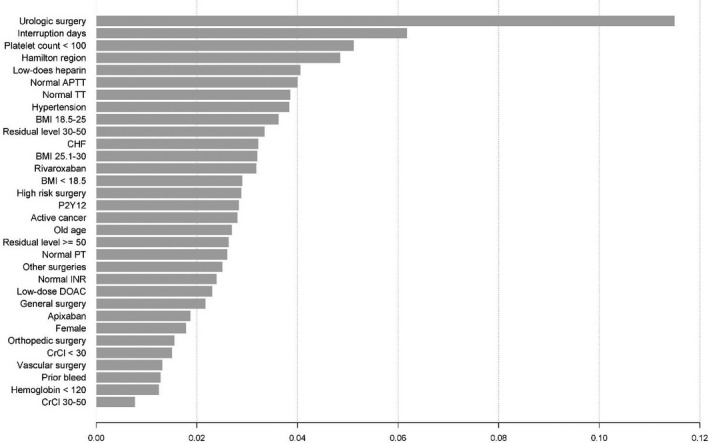
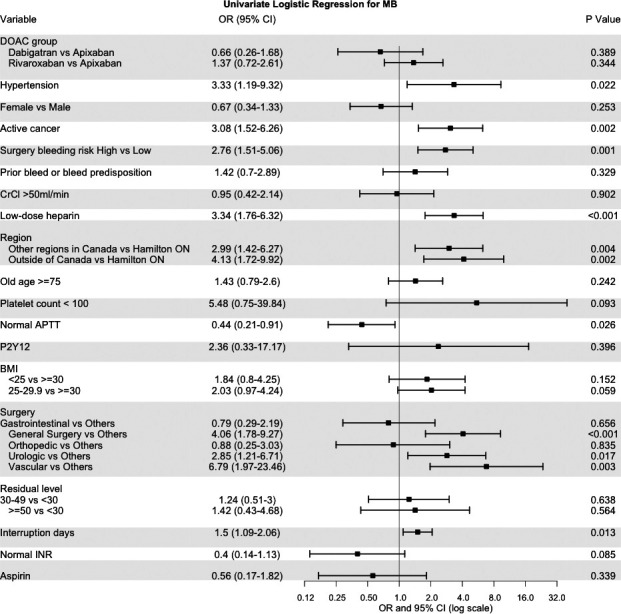
Background In the PAUSE (Perioperative Anticoagulant Use for Surgery Evaluation) Study, a simple, standardized, perioperative interruption strategy was provided for patients with nonvalvular atrial fibrillation taking direct oral anticoagulants (DOACs). Our objective was to define the factors associated with perioperative bleeding. Methods and Results We analyzed bleeding as the composite of major and clinically relevant nonmajor bleeding. Putative predictors of bleeding, and preoperative DOAC level were prospectively collected during recruitment. We used stratified logistic regression models for analysis. All statistical analyses were performed in R version 3.6.0. There were 3007 patients requiring perioperative DOAC interruption. More than one third of the included patients underwent a high bleeding risk procedure. The 30-day rates of major and clinically relevant nonmajor bleeding were 3.02% in apixaban (n=1257), 2.84% in dabigatran (n=668), and 4.16% for rivaroxaban (n=1082). Multivariate analysis stratified by region found more bleeding for hypertension (odds ratio [OR], 1.79; 95% CI 1.07-2.99; P=0.027), and prior bleeding (OR, 1.71; 95% CI, 1.08-2.71; P=0.021). Surgical bleed risk classification (high- versus low-risk) as a predictor of bleeding was only significant in the univariate analysis. The prediction model for major and clinically relevant nonmajor bleeding had an area under the curve of 0.71, and the preoperative DOAC level did not improve the area under the curve of the model. Conclusions In patients treated with DOACs who required an elective surgery/procedure and were managed with standardized DOAC interruption and resumption, there we did not find reversible risk factors for bleeding, suggesting that adjustment of the PAUSE management protocol to mitigate against bleeding is not needed.
Keywords: atrial fibrillation; bleeding; direct oral anticoagulant; surgery.
Conflict of interest statement
Dr Tafur is a consultant for Recovery Force and has received research or educational funding from: Janssen, Bristol‐Myers Squibb, Idorsia, Daichi Sanyo, Stago, and Doasesne. Dr Spyropoulos offers consultancy to Bayer, Ingelheim, Portola, Janssen; and has received research funding from Boehringer Ingelheim and Janssen. Dr. Schulman has grants and personal fees from Boehringer Ingelheim and Octapharma. In addition, he has personal fees from Bayer, Daichi Sankyo, Pfizer, Alnylam, and Sanofi. Dr. Caprini has served in a steering committee for Jansen R&D. In addition, he has served as consultant for Recovery Force, Alexion Pharmaceuticals, and has been in advisory boards for Pfizer and Sanofi. Dr Douketis has served in advisory committees for Pfizer, Sanofi, Leo Pharma, Bristol‐Myers Squibb, Portola, and Janssen. In addition, he has received a patent and royalties from The Merck Manual and Up‐to‐Date. The remaining authors have no disclosures to report.
Figures
References
-
- Spyropoulos AC, Brohi K, Caprini J, Samama CM, Siegal D, Tafur A, Verhamme P, Douketis JD. Perioperative SSCSo, Critical Care T, Haemostasis of the International Society on T and Haemostasis. Scientific and Standardization Committee Communication: Guidance document on the periprocedural management of patients on chronic oral anticoagulant therapy: Recommendations for standardized reporting of procedural/surgical bleed risk and patient‐specific thromboembolic risk. J Thromb Haemost. 2019;1966–1972. - PubMed
-
- Tafur A, Douketis J. Perioperative management of anticoagulant and antiplatelet therapy. Heart. 2018;1461–1467. - PubMed
-
- Steinberg BA, Peterson ED, Kim S, Thomas L, Gersh BJ, Fonarow GC, Kowey PR, Mahaffey KW, Sherwood MW, Chang P, et al. Outcomes Registry for Better Informed Treatment of Atrial Fibrillation I and Patients. Use and outcomes associated with bridging during anticoagulation interruptions in patients with atrial fibrillation: findings from the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT‐AF). Circulation. 2015;488–494. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
