

A Phase 2, Double-Blind, Randomized, Dose-Ranging Trial Of Reldesemtiv In Patients With ALS
- PMID: 32969758
- PMCID: PMC8117790
- DOI: 10.1080/21678421.2020.1822410
A Phase 2, Double-Blind, Randomized, Dose-Ranging Trial Of Reldesemtiv In Patients With ALS
Abstract
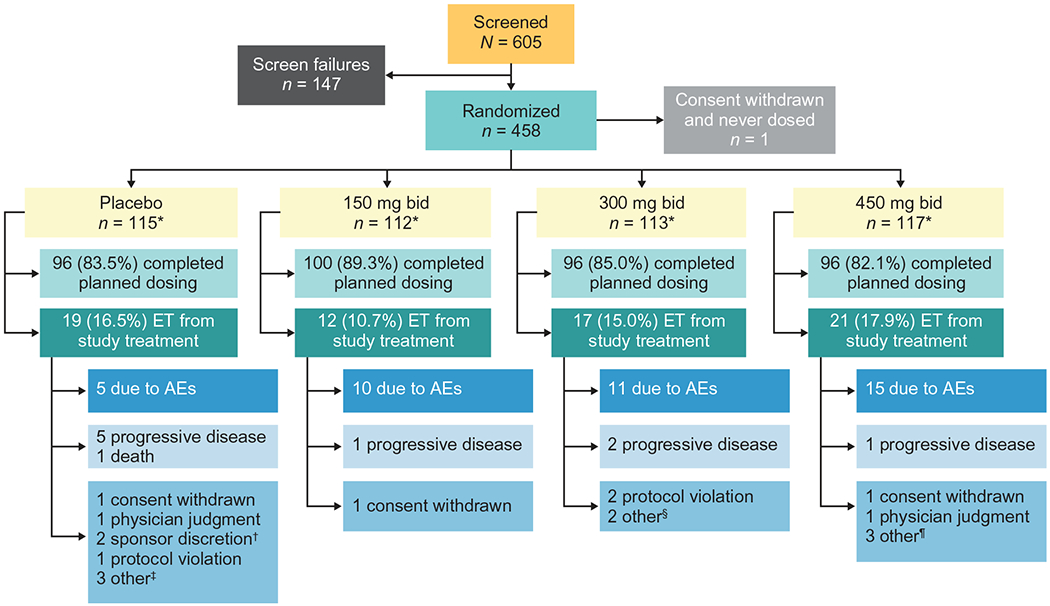
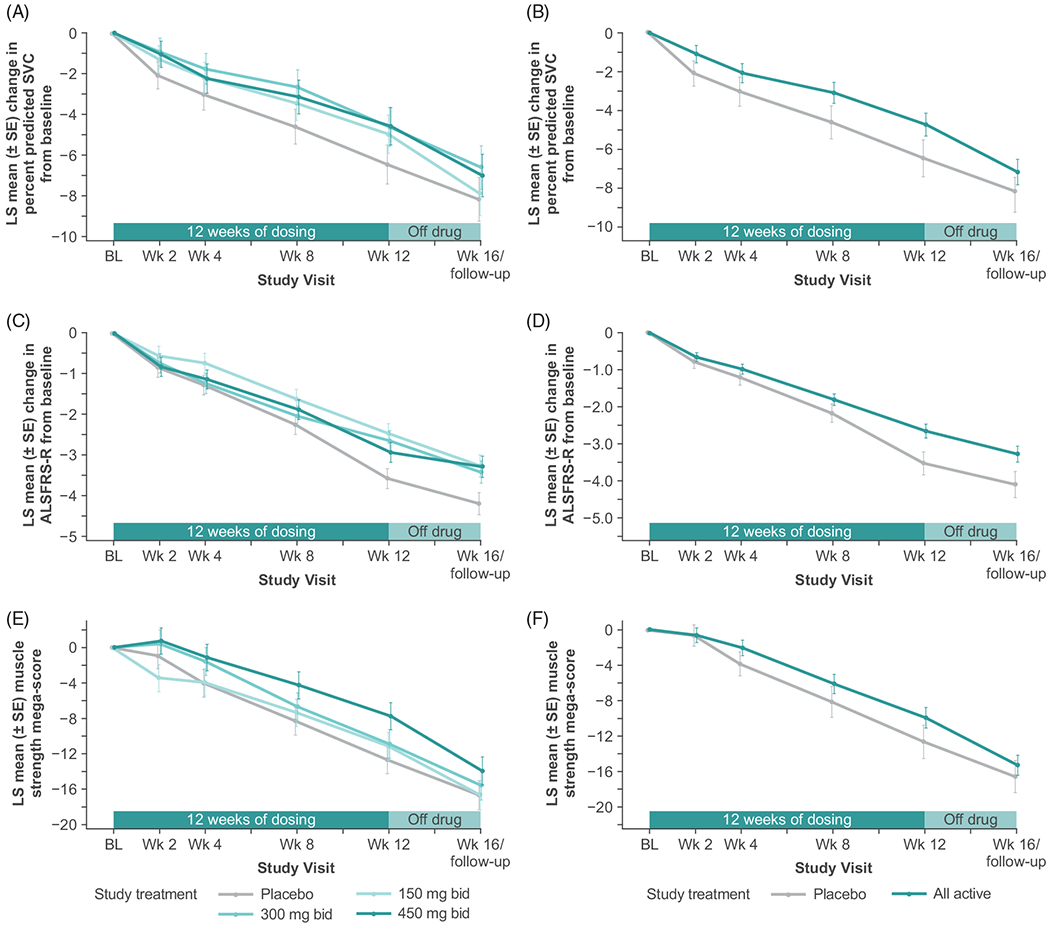
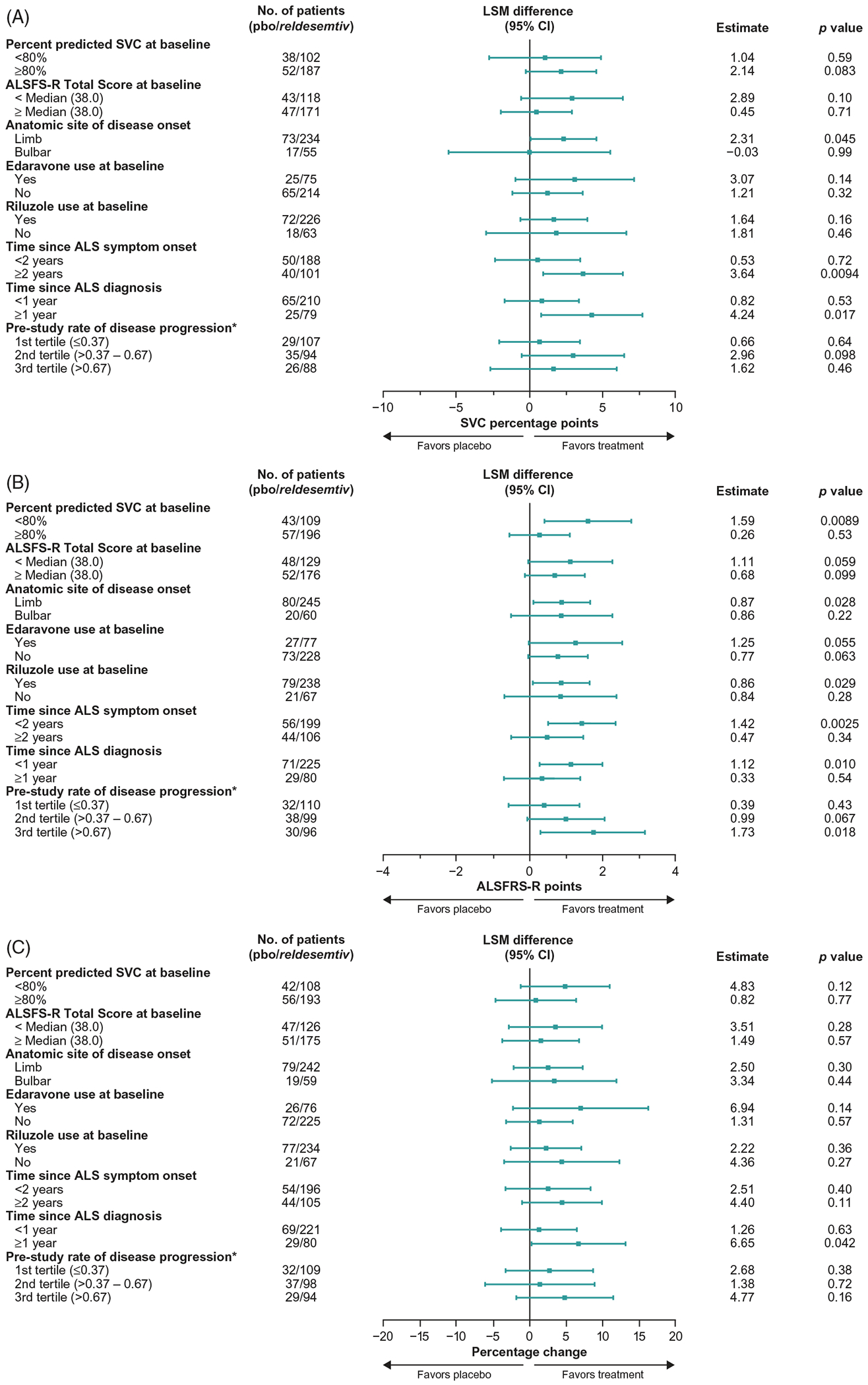
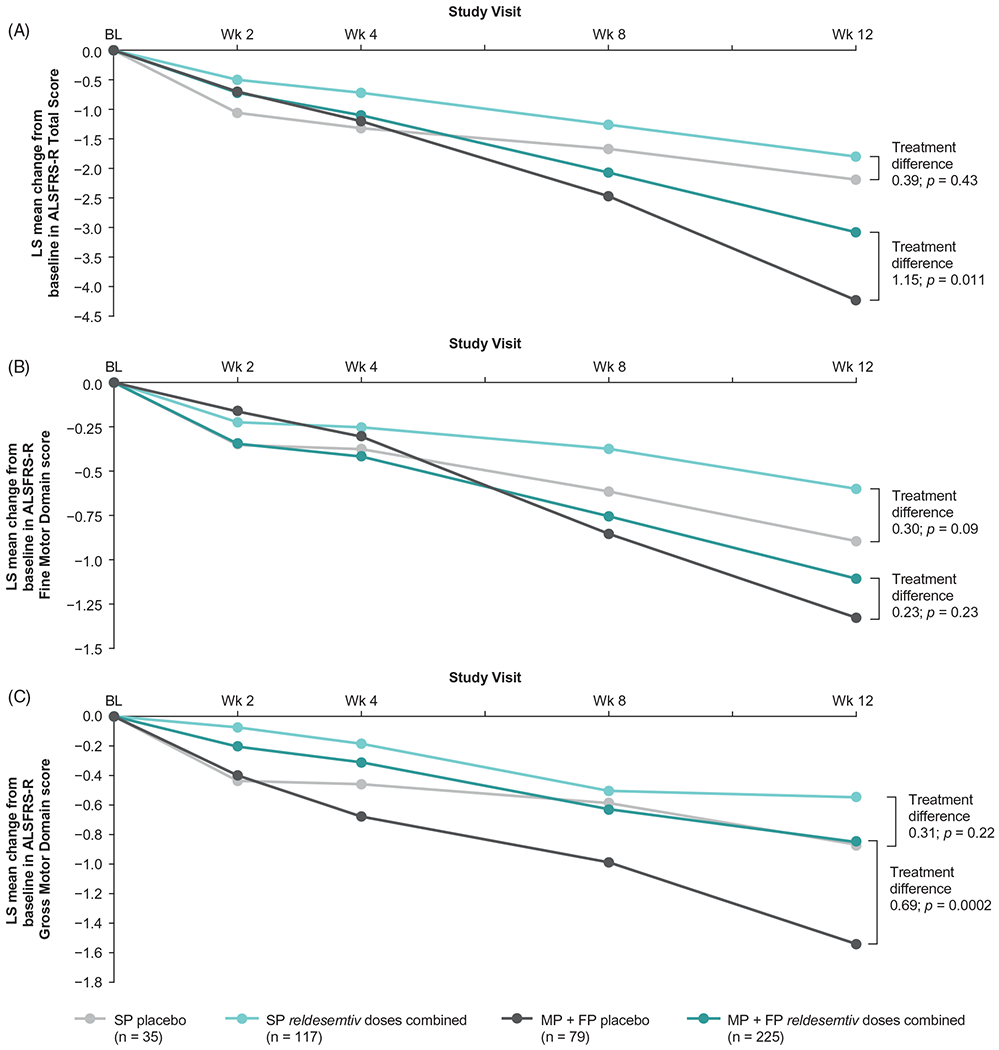
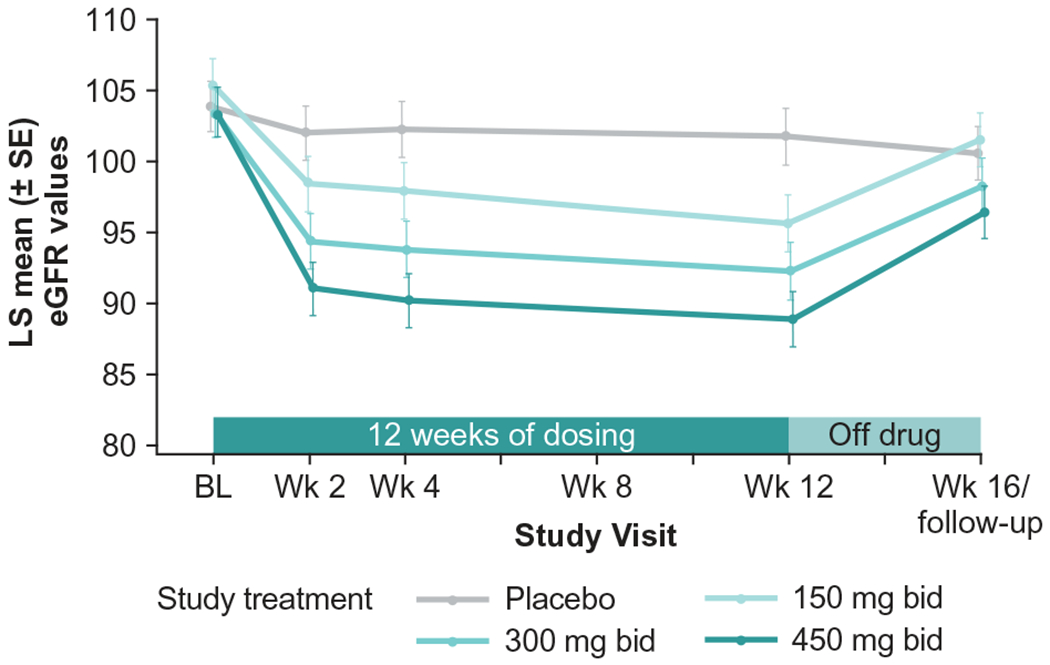
To evaluate safety, dose response, and preliminary efficacy of reldesemtiv over 12 weeks in patients with amyotrophic lateral sclerosis (ALS). Methods: Patients (≤2 years since diagnosis) with slow upright vital capacity (SVC) of ≥60% were randomized 1:1:1:1 to reldesemtiv 150, 300, or 450 mg twice daily (bid) or placebo; active treatment was 12 weeks with 4-week follow-up. Primary endpoint was change in percent predicted SVC at 12 weeks; secondary measures included ALS Functional Rating Scale-Revised (ALSFRS-R) and muscle strength mega-score. Results: Patients (N = 458) were enrolled; 85% completed 12-week treatment. The primary analysis failed to reach statistical significance (p = 0.11); secondary endpoints showed no statistically significant effects (ALSFRS-R, p = 0.09; muscle strength mega-score, p = 0.31). Post hoc analyses pooling all active reldesemtiv-treated patients compared against placebo showed trends toward benefit in all endpoints (progression rate for SVC, ALSFRS-R, and muscle strength mega-score (nominal p values of 0.10, 0.01 and 0.20 respectively)). Reldesemtiv was well tolerated, with nausea and fatigue being the most common side effects. A dose-dependent decrease in estimated glomerular filtration rate was noted, and transaminase elevations were seen in approximately 5% of patients. Both hepatic and renal abnormalities trended toward resolution after study drug discontinuation. Conclusions: Although the primary efficacy analysis did not demonstrate statistical significance, there were trends favoring reldesemtiv for all three endpoints, with effect sizes generally regarded as clinically important. Tolerability was good; modest hepatic and renal abnormalities were reversible. The impact of reldesemtiv on patients with ALS should be assessed in a pivotal Phase 3 trial. (ClinicalTrials.gov Identifier: NCT03160898).
Keywords: Randomized clinical trial; amyotrophic lateral sclerosis; reldesemtiv.
Conflict of interest statement
Declaration of interest
JMS received personal compensation from Avexis, Biogen, Brainstorm, Cytokinetics, Mitsubishi Tanabe Pharma America, Neurosense, Orphazyme, Otsuka, and Revalesio; and research support from Amylyx, Brainstorm, Cytokinetics, Medicinova, and Mitsubishi Tanabe Pharma America. JAA served as a consultant for ALS Pharma, Avexis, Biogen and Cytokinetics; is a former employee of Cytokinetics; and received research support from Biogen, Neuraltus, Orion, Roche, Novartis. AG served as a consultant for Alexion, AL-S Pharma, Biogen, Calico, and Cytokinetics. CJ has received grant support from Amylyx and Cytokinetics; served on the DSMB for Anelixis, Brainstorm, and Mallinckrodt; and served as a consultant for Cytokinetics, ITF Pharma, and Mitsubishi Tanabe Pharma America. NL is a consultant for Cytokinetics. TMM is a consultant for Cytokinetics and Disarm Therapeutics; has licensing agreements with C2N Diagnostics and Ionis Pharmaceuticals; and serves on the advisory board and receives research support from Biogen. CB served (uncompensated) on an advisory board for Argenx. BRB has received personal compensation for consulting, serving on a scientific advisory board, speaking, or other activities from AB Science, Biogen, Biohaven, California ALS Research Summit, Cytokinetics, ITF Pharma, Mitsubishi Tanabe Pharma American, and for serving in an editorial capacity for
Figures
References
-
- Shefner J, Cedarbaum JM, Cudkowicz ME, Maragakis N, Lee J, Jones D, et al. Safety, tolerability and pharmacodynamics of a skeletal muscle activator in amyotrophic lateral sclerosis. Amyotroph Lateral Scler. 2012;13:430–8. - PubMed
-
- Shefner JM, Watson ML, Meng L, Wolff AA. A study to evaluate safety and tolerability of repeated doses of tirasemtiv in patients with amyotrophic lateral sclerosis. Amyotroph Lateral Scler Frontotemporal Degener. 2013; 14:574–81. - PubMed
-
- Shefner JM, Wolff AA, Meng L. The relationship between tirasemtiv serum concentration and functional outcomes in patients with ALS. Amyotroph Lateral Scler Frontotemporal Degener. 2013;14:582–5. - PubMed
-
- Sanders DB, Rosenfeld J, Dimachkie MM, Meng L, Malik FI. A double-blinded, randomized, placebo-controlled trial to evaluate efficacy, safety, and tolerability of single doses of tirasemtiv in patients with acetylcholine receptor-binding antibody-positive myasthenia gravis. Neurotherapeutics. 2015;12:455–60. - PMC - PubMed
-
- Shefner JM, Wolff AA, Meng L, Bian A, Lee J, Barragan D, et al. A randomized, placebo-controlled, double-blind phase IIb trial evaluating the safety and efficacy of tirasemtiv in patients with amyotrophic lateral sclerosis. Amyotroph Lateral Scler Frontotemporal Degener. 2016; 17:426–35. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous