

Validation of a Machine Learning Algorithm to Predict 180-Day Mortality for Outpatients With Cancer
- PMID: 32970131
- PMCID: PMC7516810
- DOI: 10.1001/jamaoncol.2020.4331
Validation of a Machine Learning Algorithm to Predict 180-Day Mortality for Outpatients With Cancer
Abstract
Importance: Machine learning (ML) algorithms can identify patients with cancer at risk of short-term mortality to inform treatment and advance care planning. However, no ML mortality risk prediction algorithm has been prospectively validated in oncology or compared with routinely used prognostic indices.
Objective: To validate an electronic health record-embedded ML algorithm that generated real-time predictions of 180-day mortality risk in a general oncology cohort.
Design, setting, and participants: This prognostic study comprised a prospective cohort of patients with outpatient oncology encounters between March 1, 2019, and April 30, 2019. An ML algorithm, trained on retrospective data from a subset of practices, predicted 180-day mortality risk between 4 and 8 days before a patient's encounter. Patient encounters took place in 18 medical or gynecologic oncology practices, including 1 tertiary practice and 17 general oncology practices, within a large US academic health care system. Patients aged 18 years or older with outpatient oncology or hematology and oncology encounters were included in the analysis. Patients were excluded if their appointment was scheduled after weekly predictions were generated and if they were only evaluated in benign hematology, palliative care, or rehabilitation practices.
Exposures: Gradient-boosting ML binary classifier.
Main outcomes and measures: The primary outcome was the patients' 180-day mortality from the index encounter. The primary performance metric was the area under the receiver operating characteristic curve (AUC).
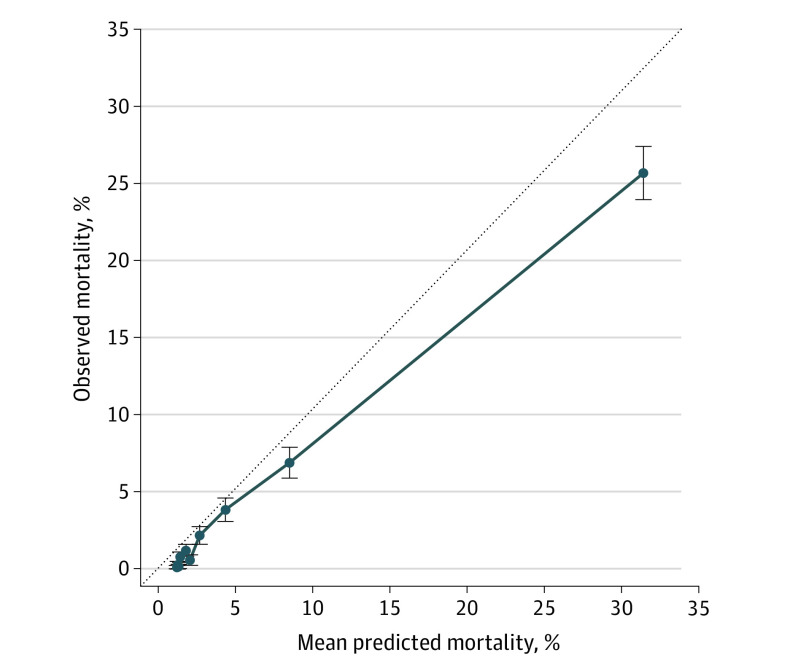
Results: Among 24 582 patients, 1022 (4.2%) died within 180 days of their index encounter. Their median (interquartile range) age was 64.6 (53.6-73.2) years, 15 319 (62.3%) were women, 18 015 (76.0%) were White, and 10 658 (43.4%) were seen in the tertiary practice. The AUC was 0.89 (95% CI, 0.88-0.90) for the full cohort. The AUC varied across disease-specific groups within the tertiary practice (AUC ranging from 0.74 to 0.96) but was similar between the tertiary and general oncology practices. At a prespecified 40% mortality risk threshold used to differentiate high- vs low-risk patients, observed 180-day mortality was 45.2% (95% CI, 41.3%-49.1%) in the high-risk group vs 3.1% (95% CI, 2.9%-3.3%) in the low-risk group. Integrating the algorithm into the Eastern Cooperative Oncology Group and Elixhauser comorbidity index-based classifiers resulted in favorable reclassification (net reclassification index, 0.09 [95% CI, 0.04-0.14] and 0.23 [95% CI, 0.20-0.27], respectively).
Conclusions and relevance: In this prognostic study, an ML algorithm was feasibly integrated into the electronic health record to generate real-time, accurate predictions of short-term mortality for patients with cancer and outperformed routinely used prognostic indices. This algorithm may be used to inform behavioral interventions and prompt earlier conversations about goals of care and end-of-life preferences among patients with cancer.
Conflict of interest statement
Figures

Comment in
-
Closing the Gap Between Machine Learning and Clinical Cancer Care-First Steps Into a Larger World.JAMA Oncol. 2020 Nov 1;6(11):1731-1732. doi: 10.1001/jamaoncol.2020.4314. JAMA Oncol. 2020. PMID: 32970129 No abstract available.
Similar articles
-
Machine Learning Approaches to Predict 6-Month Mortality Among Patients With Cancer.JAMA Netw Open. 2019 Oct 2;2(10):e1915997. doi: 10.1001/jamanetworkopen.2019.15997. JAMA Netw Open. 2019. PMID: 31651973 Free PMC article.
-
Effect of Integrating Machine Learning Mortality Estimates With Behavioral Nudges to Clinicians on Serious Illness Conversations Among Patients With Cancer: A Stepped-Wedge Cluster Randomized Clinical Trial.JAMA Oncol. 2020 Dec 1;6(12):e204759. doi: 10.1001/jamaoncol.2020.4759. Epub 2020 Dec 10. JAMA Oncol. 2020. PMID: 33057696 Free PMC article. Clinical Trial.
-
Development and Application of a Machine Learning Approach to Assess Short-term Mortality Risk Among Patients With Cancer Starting Chemotherapy.JAMA Netw Open. 2018 Jul 6;1(3):e180926. doi: 10.1001/jamanetworkopen.2018.0926. JAMA Netw Open. 2018. PMID: 30646043 Free PMC article.
-
Long-term Effect of Machine Learning-Triggered Behavioral Nudges on Serious Illness Conversations and End-of-Life Outcomes Among Patients With Cancer: A Randomized Clinical Trial.JAMA Oncol. 2023 Mar 1;9(3):414-418. doi: 10.1001/jamaoncol.2022.6303. JAMA Oncol. 2023. PMID: 36633868 Free PMC article. Clinical Trial.
-
Machine Learning-Based Short-Term Mortality Prediction Models for Patients With Cancer Using Electronic Health Record Data: Systematic Review and Critical Appraisal.JMIR Med Inform. 2022 Mar 14;10(3):e33182. doi: 10.2196/33182. JMIR Med Inform. 2022. PMID: 35285816 Free PMC article. Review.
Cited by
-
Machine learning methods to predict presence of residual cancer following hysterectomy.Sci Rep. 2022 Feb 17;12(1):2738. doi: 10.1038/s41598-022-06585-x. Sci Rep. 2022. PMID: 35177700 Free PMC article.
-
Applications of Machine Learning in Palliative Care: A Systematic Review.Cancers (Basel). 2023 Mar 4;15(5):1596. doi: 10.3390/cancers15051596. Cancers (Basel). 2023. PMID: 36900387 Free PMC article. Review.
-
Prospective Comparison of Medical Oncologists and a Machine Learning Model to Predict 3-Month Mortality in Patients With Metastatic Solid Tumors.JAMA Netw Open. 2022 May 2;5(5):e2214514. doi: 10.1001/jamanetworkopen.2022.14514. JAMA Netw Open. 2022. PMID: 35639380 Free PMC article.
-
Artificial intelligence across oncology specialties: current applications and emerging tools.BMJ Oncol. 2024 Jan 17;3(1):e000134. doi: 10.1136/bmjonc-2023-000134. eCollection 2024. BMJ Oncol. 2024. PMID: 39886165 Free PMC article. Review.
-
Performance of electronic medical record tool in predicting 6-month mortality in hospitalized patients with cancer.J Hosp Med. 2025 Aug;20(8):829-836. doi: 10.1002/jhm.70012. Epub 2025 Feb 17. J Hosp Med. 2025. PMID: 39961789 Free PMC article.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
