

Early predictors of in-hospital mortality in patients with COVID-19 in a large American cohort
- PMID: 32970246
- PMCID: PMC7512216
- DOI: 10.1007/s11739-020-02509-7
Early predictors of in-hospital mortality in patients with COVID-19 in a large American cohort
Abstract
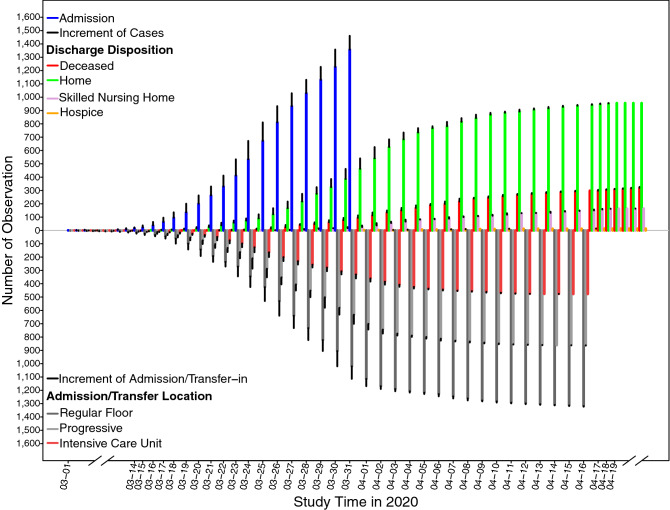
Coronavirus disease (COVID-19) has aggressively spread across the United States with numerous fatalities. Risk factors for mortality are poorly described. This was a multicentered cohort study identifying patient characteristics and diagnostic markers present on initial evaluation associated with mortality in hospitalized COVID-19 patients. Epidemiological, demographic, clinical, and laboratory characteristics of survivors and non-survivors were obtained from electronic medical records and a multivariable survival regression analysis was conducted to identify risk factors of in-hospital death. Of 1629 consecutive hospitalized adult patients with confirmed COVID-19 from March 1st thru March 31, 2020, 1461 patients were included in final analysis. 327 patients died during hospitalization and 1134 survived to discharge. Median age was 62 years (IQR 50.0, 74.0) with 56% of hospitalized patients under the age of 65. 47% were female and 63% identified as African American. Most patients (55%) had either no or one comorbidity. In multivariable analysis, older age, admission respiratory status including elevated respiratory rate and oxygen saturation ≤ 88%, and initial laboratory derangements of creatinine > 1.33 mg/dL, alanine aminotransferase > 40 U/L, procalcitonin > 0.5 ng/mL, and lactic acid ≥ 2 mmol/L increased risk of in-hospital death. This study is one of the largest analyses in an epicenter for the COVID-19 pandemic. Older age, low oxygen saturation and elevated respiratory rate on admission, and initial lab derangements including renal and hepatic dysfunction and elevated procalcitonin and lactic acid are risk factors for in-hospital death. These factors can help clinicians prognosticate and should be considered in management strategies.
Keywords: COVID-19; Mortality; Predictors; Scoring system.
Conflict of interest statement
This manuscript in part or in full has not been submitted or published anywhere. No authors have any relevant conflict of interest disclosures.
Figures


References
-
- World Health Organization (2020) Novel coronavirus—China. January 12, 2020 . Geneva: World Health Organization. https://www.who.int/csr/don/12-january-2020-novel-coronavirus-china/en/. Accessed 30 Apr 2020
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
