

Heterogeneous expression of the SARS-Coronavirus-2 receptor ACE2 in the human respiratory tract
- PMID: 32971472
- PMCID: PMC7505653
- DOI: 10.1016/j.ebiom.2020.102976
Heterogeneous expression of the SARS-Coronavirus-2 receptor ACE2 in the human respiratory tract
Abstract
Background: Zoonotically transmitted coronaviruses are responsible for three disease outbreaks since 2002, including the current COVID-19 pandemic, caused by SARS-CoV-2. Its efficient transmission and range of disease severity raise questions regarding the contributions of virus-receptor interactions. ACE2 is a host ectopeptidase and the receptor for SARS-CoV-2. Numerous reports describe ACE2 mRNA abundance and tissue distribution; however, mRNA abundance is not always representative of protein levels. Currently, there is limited data evaluating ACE2 protein and its correlation with other SARS-CoV-2 susceptibility factors.
Materials and methods: We systematically examined the human upper and lower respiratory tract using single-cell RNA sequencing and immunohistochemistry to determine receptor expression and evaluated its association with risk factors for severe COVID-19.
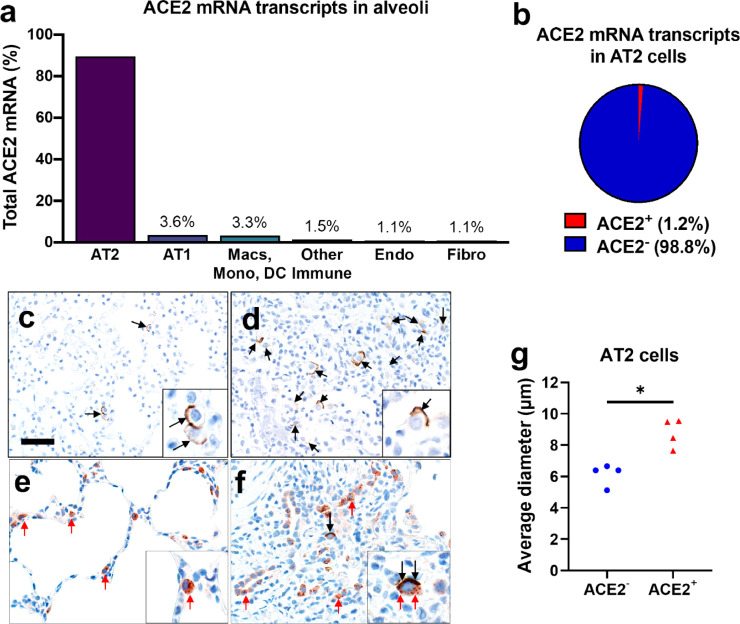
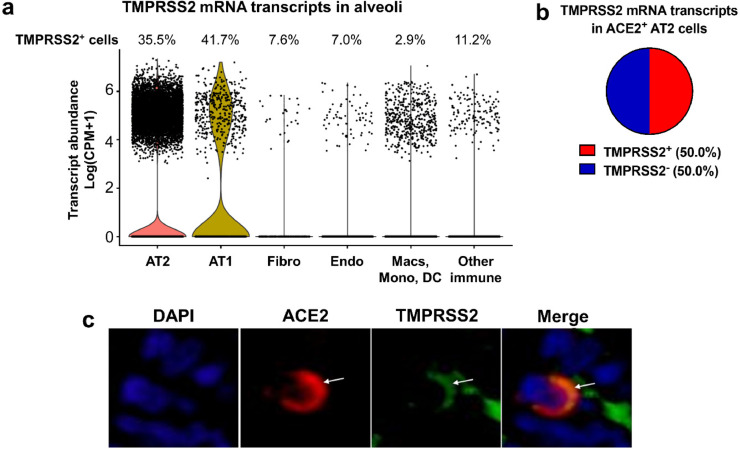
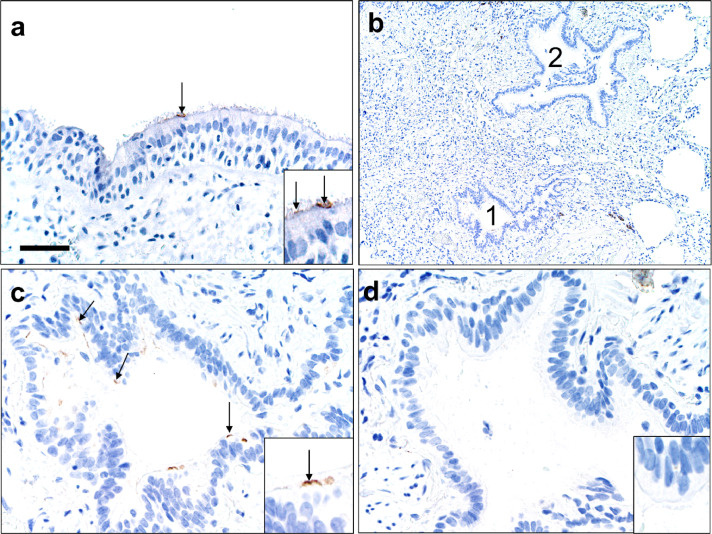
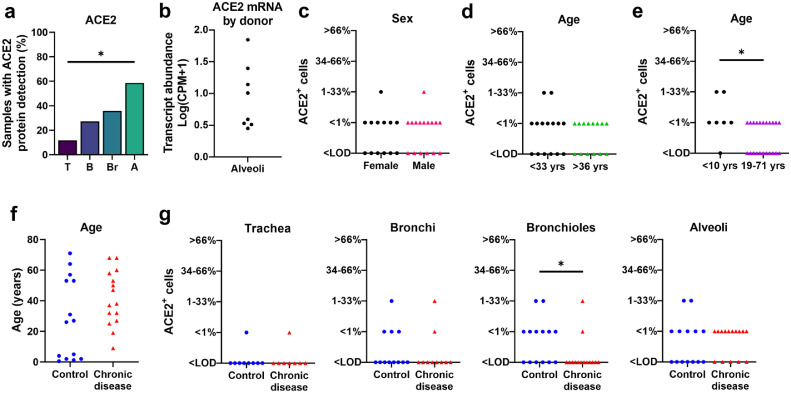
Findings: Our results reveal that ACE2 protein is highest within regions of the sinonasal cavity and pulmonary alveoli, sites of presumptive viral transmission and severe disease development, respectively. In the lung parenchyma, ACE2 protein was found on the apical surface of a small subset of alveolar type II cells and colocalized with TMPRSS2, a cofactor for SARS-CoV2 entry. ACE2 protein was not increased by pulmonary risk factors for severe COVID-19. Additionally, ACE2 protein was not reduced in children, a demographic with a lower incidence of severe COVID-19.
Interpretation: These results offer new insights into ACE2 protein localization in the human respiratory tract and its relationship with susceptibility factors to COVID-19.
Keywords: Alveolar type II cells; Ciliated cells; Expression; Immunohistochemistry; Lung.
Copyright © 2020 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare no competing interests related to this work. This work was supported by the National Institutes of Health (NIH, P01 AI060699). P.B.M. is on the scientific advisory board and receives support for sponsored research from Spirovant Sciences, Inc. P.B.M. is on the scientific advisory board for Oryn Therapeutics.
Figures
Update of
-
Heterogeneous expression of the SARS-Coronavirus-2 receptor ACE2 in the human respiratory tract.bioRxiv [Preprint]. 2020 Aug 13:2020.04.22.056127. doi: 10.1101/2020.04.22.056127. bioRxiv. 2020. Update in: EBioMedicine. 2020 Oct;60:102976. doi: 10.1016/j.ebiom.2020.102976. PMID: 32577664 Free PMC article. Updated. Preprint.
Comment in
-
Differential expression of ACE2 in the respiratory tracts and its relationship to COVID-19 pathogenesis.EBioMedicine. 2020 Oct;60:103004. doi: 10.1016/j.ebiom.2020.103004. Epub 2020 Sep 24. EBioMedicine. 2020. PMID: 32979833 Free PMC article. No abstract available.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
