

Geographical Variation in the Use of Diverting Loop Ileostomy in Australia and New Zealand Colorectal Surgeons
- PMID: 32972099
- PMCID: PMC8566141
- DOI: 10.3393/ac.2020.09.14.1
Geographical Variation in the Use of Diverting Loop Ileostomy in Australia and New Zealand Colorectal Surgeons
Abstract
Purpose: Anastomotic leak (AL) after a low pelvic anastomosis is a devastating complication, with short- and long-term morbidity and increased mortality. Surgeons may employ various adjuncts in an attempt to reduce AL rates or mitigate their impact. These include the use of temporary diverting ileostomy (TDI), transanal or rectal tubes and pelvic drains. This questionnaire evaluates the preferences and routine use of these adjuncts in Australasian colorectal surgeons.
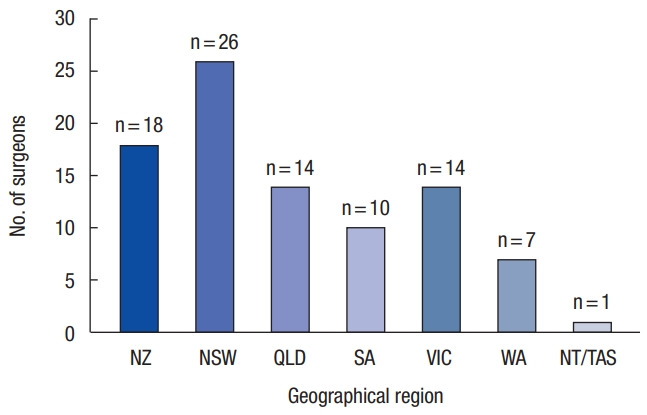
Methods: A cross-sectional survey was administered to Australian and New Zealand colorectal surgeons on September 20, 2018. The study survey consisted of 15 questions exploring basic demographics and the number of rectal resections and ileal pouches performed in 12 months, along with the surgeon's preference for the use of diverting stomas, rectal tubes, and pelvic drains.
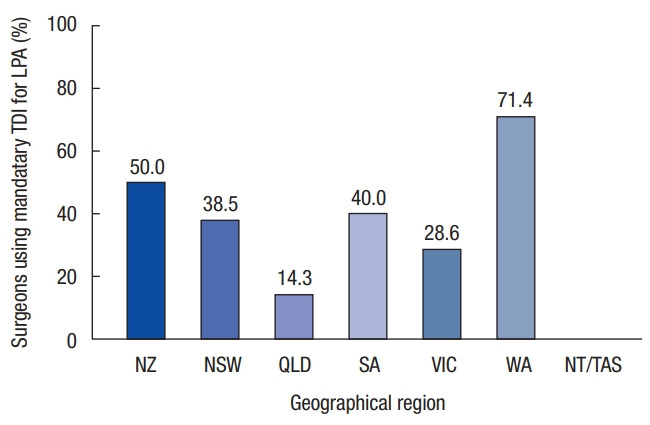
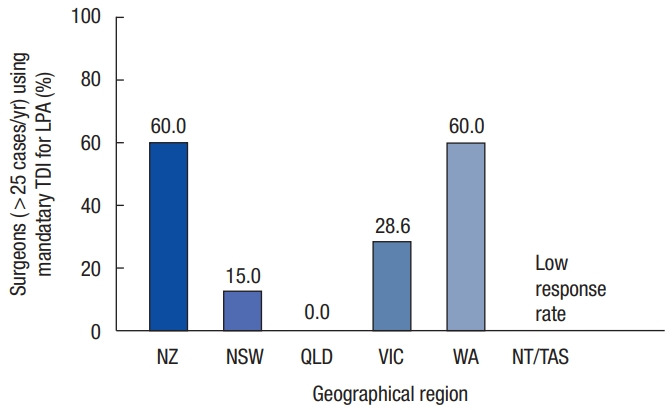
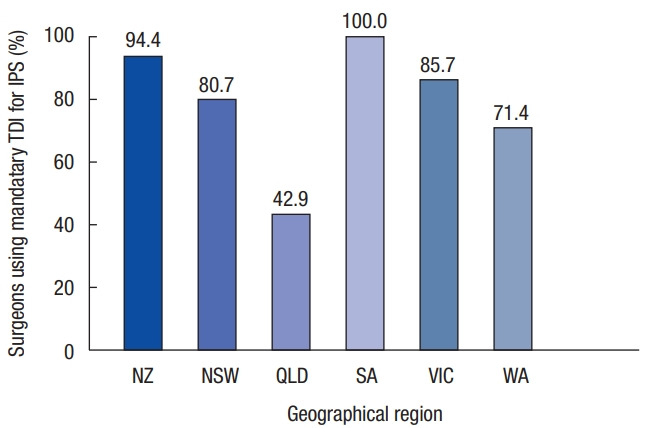
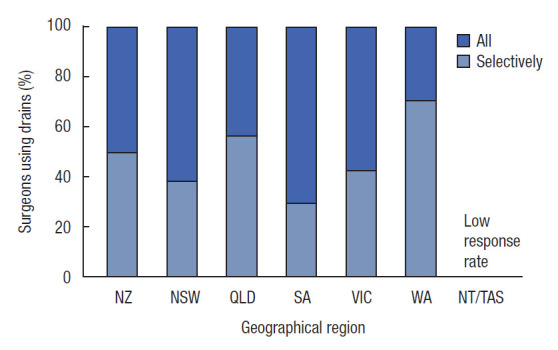
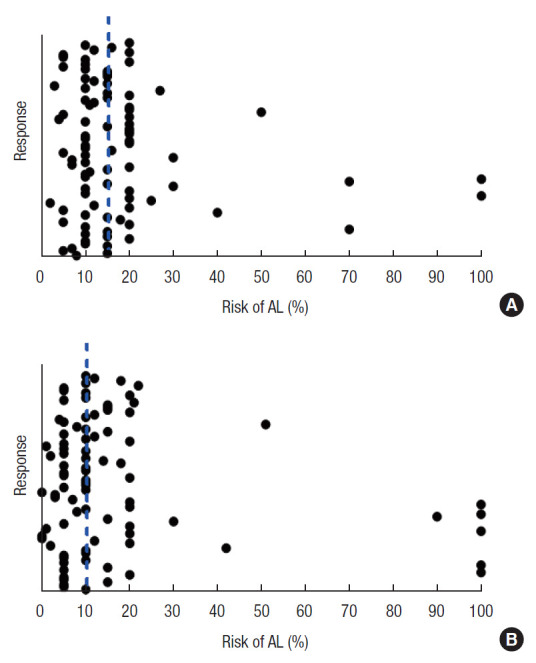
Results: There were 90 respondents to the survey (31.6%). Surgeons in Western Australia (71.4%) were more likely to use a mandatory TDI in colorectal extraperitoneal anastomoses than surgeons in Queensland (14.3%). South Australian surgeons are more likely to employ a mandatory TDI (100%) for ileal pouches than Queensland surgeons (42.9%). Rectal tubes are not commonly utilized (40.0% never use them), and pelvic drains are (45.6% in all cases). Surgeons consider a median AL rate of 15% was felt to justify the use of a TDI in low pelvic anastomoses and a median AL rate of 10% for ileal pouches.
Conclusion: There is considerable geographical variation in colorectal surgical practice throughout Australia and New Zealand. While surgeons interrogate the same literature, there are presumably other factors that see translation into variations in clinical practice.
Keywords: Anastomotic leak; Ileostomy; Pelvic drain; Restorative proctocolectomy; Trans anal tube.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Risk taking propensity: Nurse, surgeon and patient preferences for diverting ileostomy.Colorectal Dis. 2022 Sep;24(9):1073-1079. doi: 10.1111/codi.16149. Epub 2022 May 4. Colorectal Dis. 2022. PMID: 35426482 Free PMC article.
-
Proximal diversion at the time of ileal pouch-anal anastomosis for ulcerative colitis: current practices of North American colorectal surgeons.Dis Colon Rectum. 2009 Jun;52(6):1178-83. doi: 10.1007/DCR.0b013e31819f24fc. Dis Colon Rectum. 2009. PMID: 19581865
-
Diverting ileostomy in colorectal surgery: when is it necessary?Langenbecks Arch Surg. 2015 Feb;400(2):145-52. doi: 10.1007/s00423-015-1275-1. Epub 2015 Jan 30. Langenbecks Arch Surg. 2015. PMID: 25633276 Review.
-
Routine Virtual Ileostomy Following Restorative Proctocolectomy for Familial Adenomatous Polyposis.World J Surg. 2018 Jun;42(6):1867-1871. doi: 10.1007/s00268-017-4365-0. World J Surg. 2018. PMID: 29147895
-
Restorative proctocolectomy without diverting ileostomy.Dis Colon Rectum. 1995 Feb;38(2):188-94. doi: 10.1007/BF02052449. Dis Colon Rectum. 1995. PMID: 7851175 Review.
Cited by
-
Drain fluid iodine as a biomarker of anastomotic leak after low anterior resection in patients undergoing Gastrografin rectal tube flushes and omission of a diverting ileostomy: The GUSH study.Colorectal Dis. 2025 Feb;27(2):e70031. doi: 10.1111/codi.70031. Colorectal Dis. 2025. PMID: 39973087 Free PMC article.
-
Risk taking propensity: Nurse, surgeon and patient preferences for diverting ileostomy.Colorectal Dis. 2022 Sep;24(9):1073-1079. doi: 10.1111/codi.16149. Epub 2022 May 4. Colorectal Dis. 2022. PMID: 35426482 Free PMC article.
References
-
- Boccola MA, Buettner PG, Rozen WM, Siu SK, Stevenson AR, Stitz R, et al. Risk factors and outcomes for anastomotic leakage in colorectal surgery: a single-institution analysis of 1576 patients. World J Surg. 2011;35:186–95. - PubMed
-
- Shogan BD, Carlisle EM, Alverdy JC, Umanskiy K. Do we really know why colorectal anastomoses leak? J Gastrointest Surg. 2013;17:1698–707. - PubMed
-
- Sagar PM, Pemberton JH. Intraoperative, postoperative and reoperative problems with ileoanal pouches. Br J Surg. 2012;99:454–68. - PubMed
-
- Xiao L, Zhang WB, Jiang PC, Bu XF, Yan Q, Li H, et al. Can transanal tube placement after anterior resection for rectal carcinoma reduce anastomotic leakage rate? A single-institution prospective randomized study. World J Surg. 2011;35:1367–77. - PubMed
LinkOut - more resources
Full Text Sources
