

Ileal Pouch-Anal Anastomosis for Ulcerative Colitis: An Australian Institution's Experience
- PMID: 32972106
- PMCID: PMC8566152
- DOI: 10.3393/ac.2020.08.26
Ileal Pouch-Anal Anastomosis for Ulcerative Colitis: An Australian Institution's Experience
Abstract
Purpose: We report outcomes and evaluate patient factors and the impact of surgical evolution on outcomes in consecutive ulcerative colitis patients who had restorative proctocolectomy with ileal pouch-anal anastomosis (IPAA) at an Australian institution over 26 years.
Methods: Data including clinical characteristics, preoperative medical therapy, and surgical outcomes were collected. We divided eligible patients into 3 period arms (period 1, 1990 to 1999; period 2, 2000 to 2009; period 3, 2010 to 2016). Outcomes of interest were IPAA leak and pouch failure.
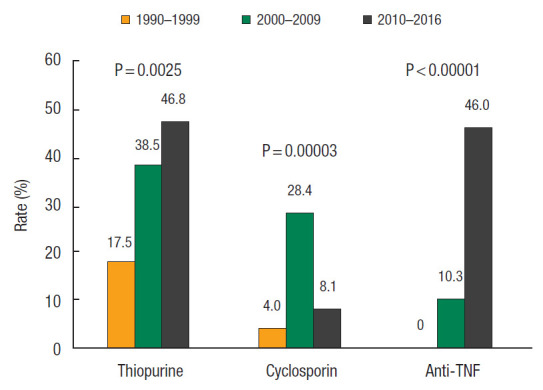
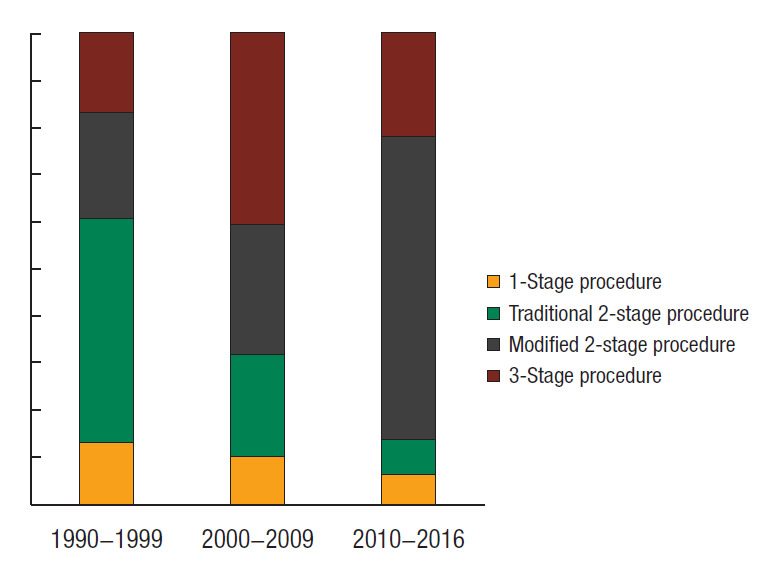
Results: A total of 212 patients were included. Median follow-up was 50 (interquartile range, 17 to 120) months. Rates of early and late complications were 34.9% and 52.0%, respectively. Early complications included wound infection (9.4%), pelvic sepsis (8.0%), and small bowel obstruction (6.6%) while late complications included small bowel obstruction (18.9%), anal stenosis (16.8%), and pouch fistula (13.3%). Overall, IPAA leak rate was 6.1% and pouch failure rate was 4.8%. Eighty-three patients (42.3%) experienced pouchitis. Over time, we observed an increase in patient exposure to thiopurine (P=0.0025), cyclosporin (P=0.0002), and anti-tumor necrosis factor (P<0.00001) coupled with a shift to laparoscopic technique (P<0.00001), stapled IPAA (P<0.00001), J pouch configuration (P<0.00001), a modified 2-stage procedure (P=0.00012), and a decline in defunctioning ileostomy rate at time of IPAA (P=0.00002). Apart from pouchitis, there was no significant difference in surgical and chronic inflammatory pouch outcomes with time.
Conclusion: Despite greater patient exposure to immunomodulatory and biologic therapy before surgery coupled with a significant change in surgical techniques, surgical and chronic inflammatory pouch outcome rates have remained stable.
Keywords: Ileal pouch-anal anastomosis; Ulcerative colitis.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Langholz E, Munkholm P, Davidsen M, Binder V. Course of ulcerative colitis: analysis of changes in disease activity over years. Gastroenterology. 1994;107:3–11. - PubMed
-
- Aratari A, Papi C, Clemente V, Moretti A, Luchetti R, Koch M, et al. Colectomy rate in acute severe ulcerative colitis in the infliximab era. Dig Liver Dis. 2008;40:821–6. - PubMed
-
- Becker JM. Ileal pouch-anal anastomosis: current status and controversies. Surgery. 1993;113:599–602. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
