

Ventilator Liberation in the Pediatric ICU
- PMID: 32973103
- PMCID: PMC8018879
- DOI: 10.4187/respcare.07810
Ventilator Liberation in the Pediatric ICU
Abstract
Despite the accepted importance of minimizing time on mechanical ventilation, only limited guidance on weaning and extubation is available from the pediatric literature. A significant proportion of patients being evaluated for weaning are actually ready for extubation, suggesting that weaning is often not considered early enough in the course of ventilation. Indications for extubation are often not clear, although a trial of spontaneous breathing on CPAP without pressure support seems an appropriate prerequisite in many cases. Several indexes have been developed to predict weaning and extubation success, but the available literature suggests they offer little or no improvement over clinical judgment. New techniques for assessing readiness for weaning and predicting extubation success are being developed but are far from general acceptance in pediatric practice. While there have been some excellent physiologic, observational, and even randomized controlled trials on aspects of pediatric ventilator liberation, robust research data are lacking. Given the lack of data in many areas, a determined approach that combines systematic review with consensus opinion of international experts could generate high-quality recommendations and terminology definitions to guide clinical practice and highlight important areas for future research in weaning, extubation readiness, and liberation from mechanical ventilation following pediatric respiratory failure.
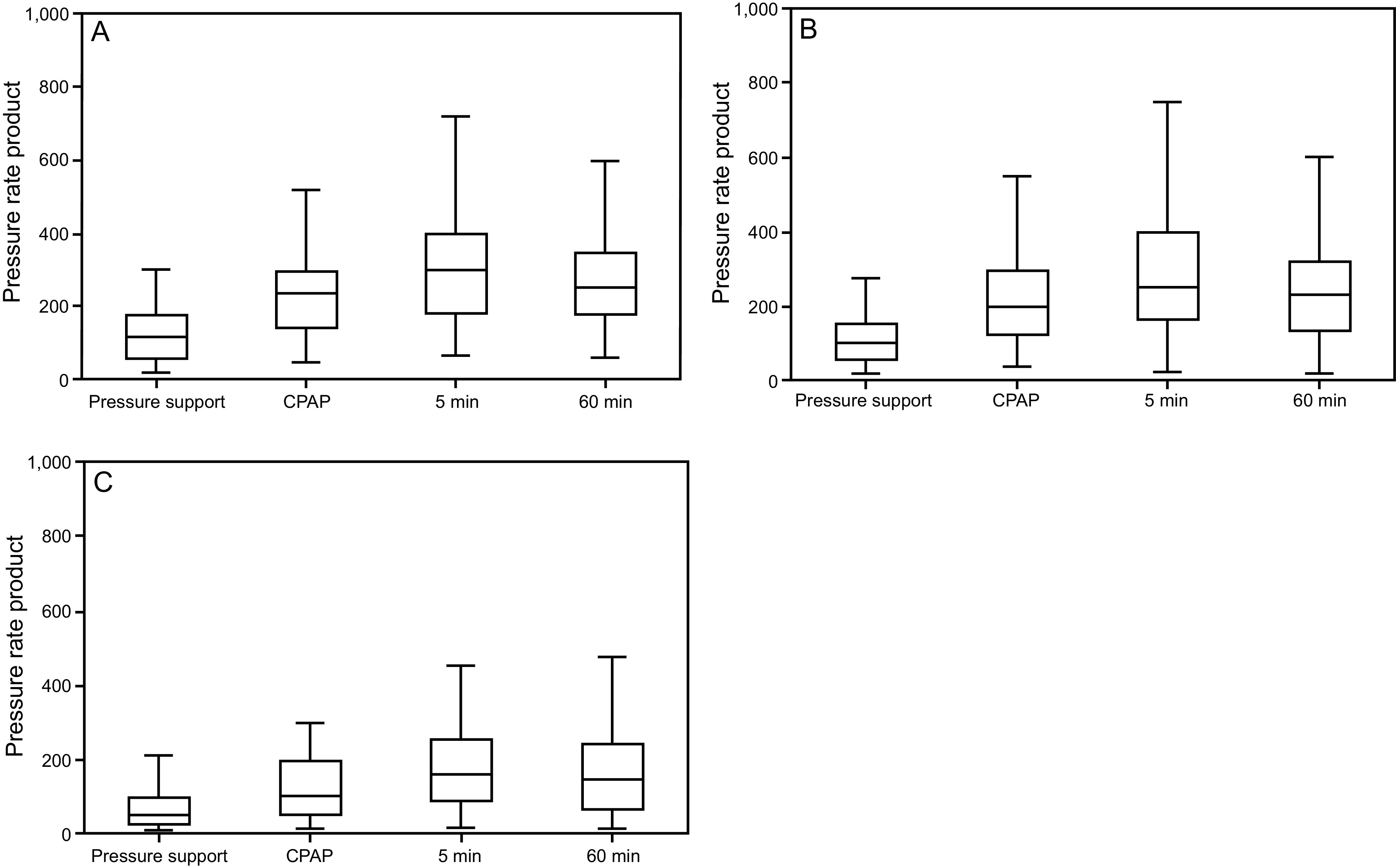
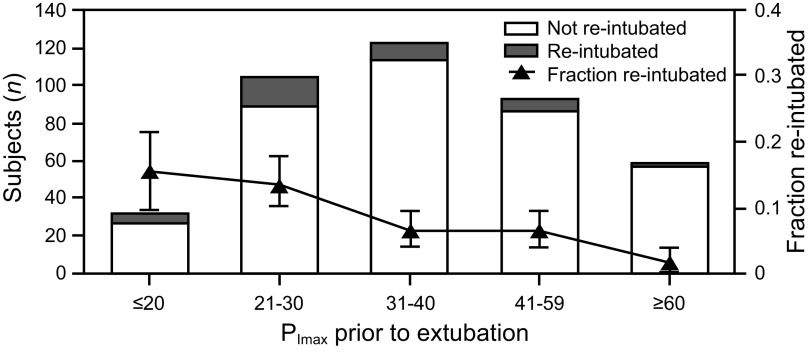
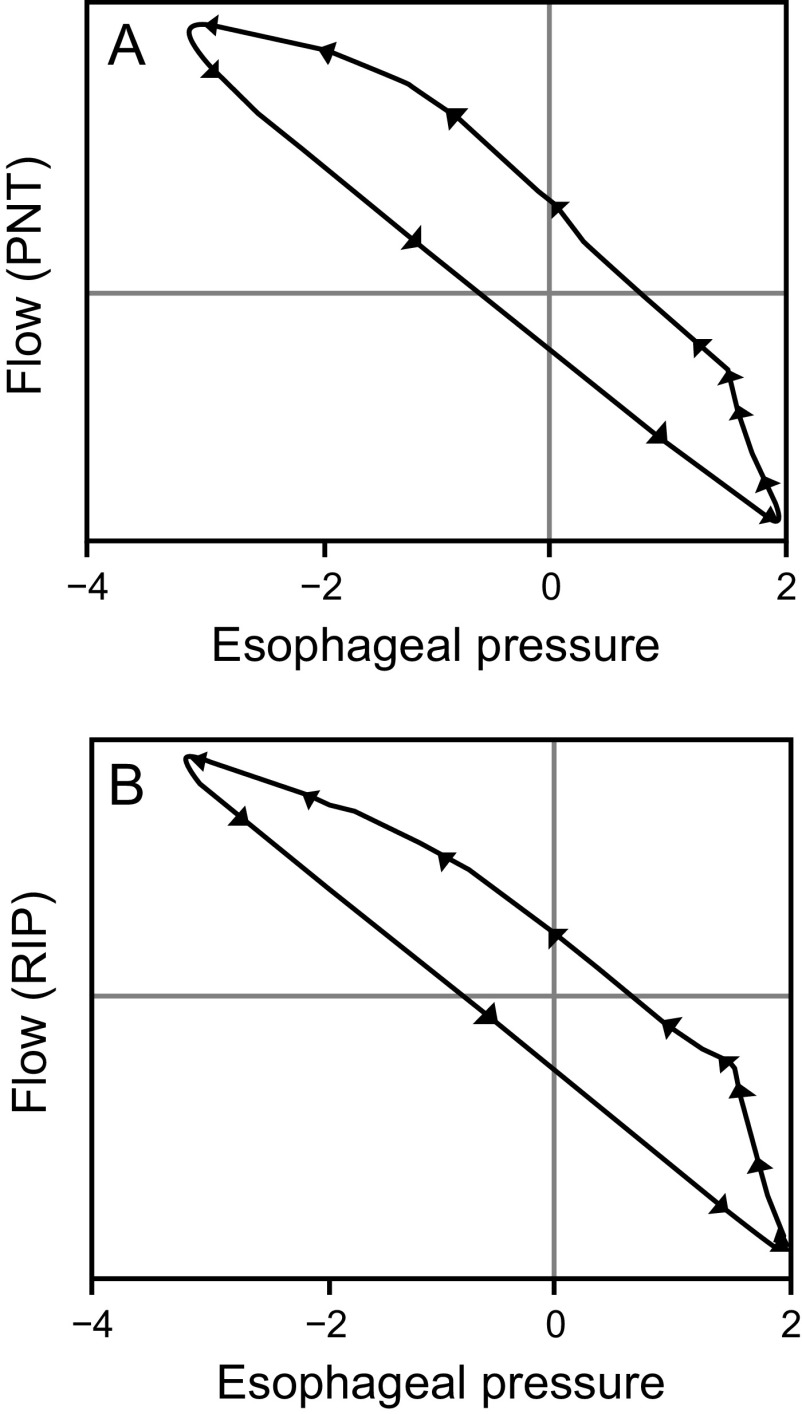
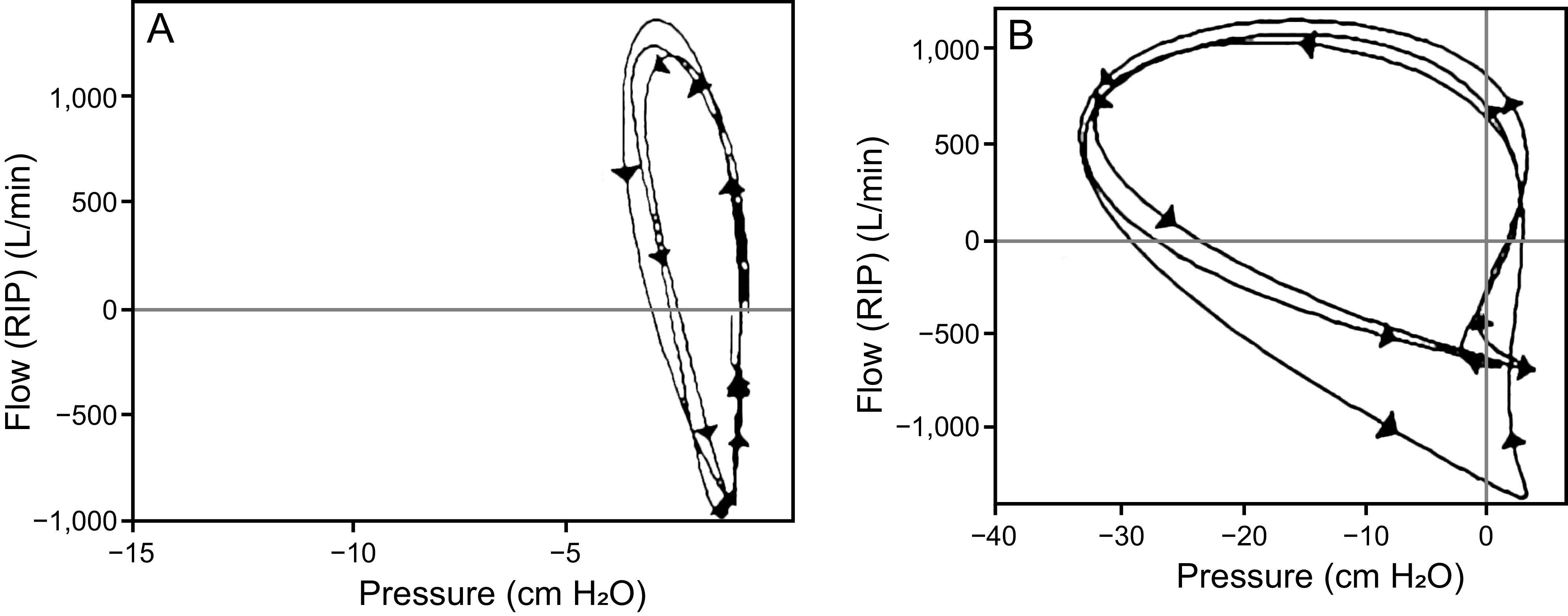
Keywords: esophageal pressure measurements; extubation; maximum negative airway pressure; mechanical ventilation; phase angles; pressure rate product; respiratory inductance plethysmography; respiratory support; spontaneous breathing; stridor; weaning.
Copyright © 2020 by Daedalus Enterprises.
Conflict of interest statement
The authors have disclosed no conflicts of interest.
Figures
References
-
- Rimensberger PC, Cheifetz IM, Kneyber M. The top ten unknowns in paediatric mechanical ventilation. Intensive Care Med 2018;44(3):366-370. - PubMed
-
- Wiedemann HP, Wheeler AP, Bernard GR, Thompson BT, Hayden D, deBoisblanc B, et al. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med 2006;354(24):2564-2575. - PubMed
-
- Ware LB, Matthay MA. Alveolar fluid clearance is impaired in the majority of patients with acute lung injury and the acute respiratory distress syndrome. Am J Respir Crit Care Med 2001;163(6):1376-1383. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
