

Retrospective unbiased plasma lipidomic of progressive multiple sclerosis patients-identifies lipids discriminating those with faster clinical deterioration
- PMID: 32973249
- PMCID: PMC7515876
- DOI: 10.1038/s41598-020-72654-8
Retrospective unbiased plasma lipidomic of progressive multiple sclerosis patients-identifies lipids discriminating those with faster clinical deterioration
Abstract
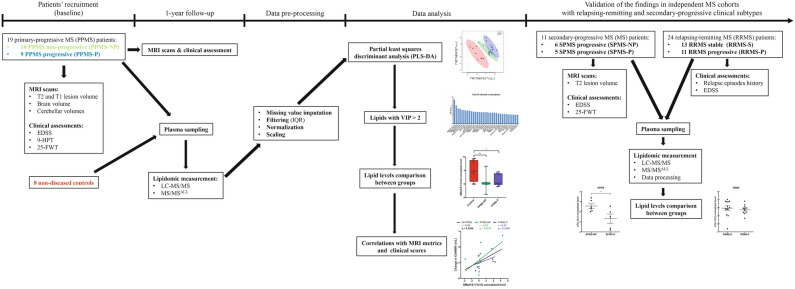
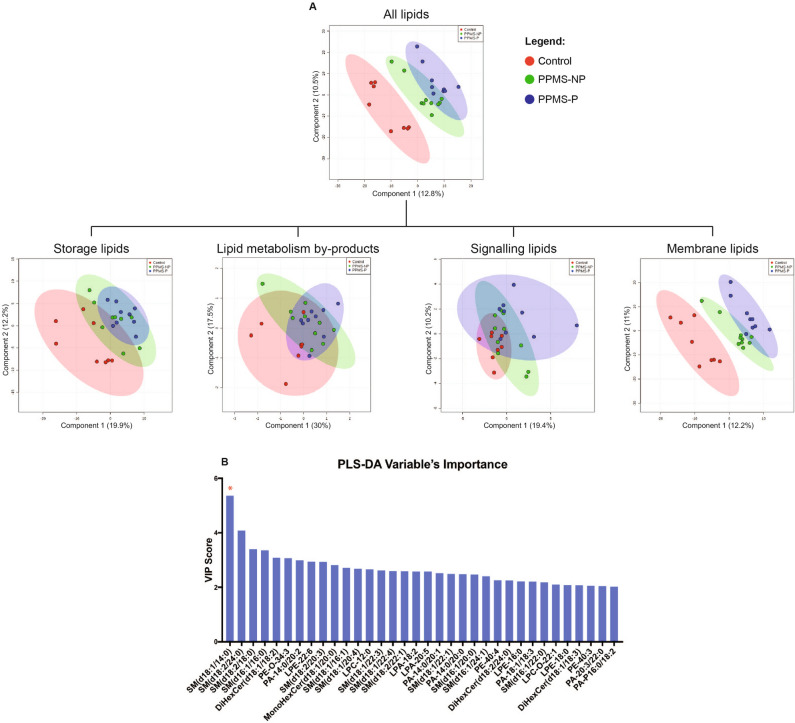
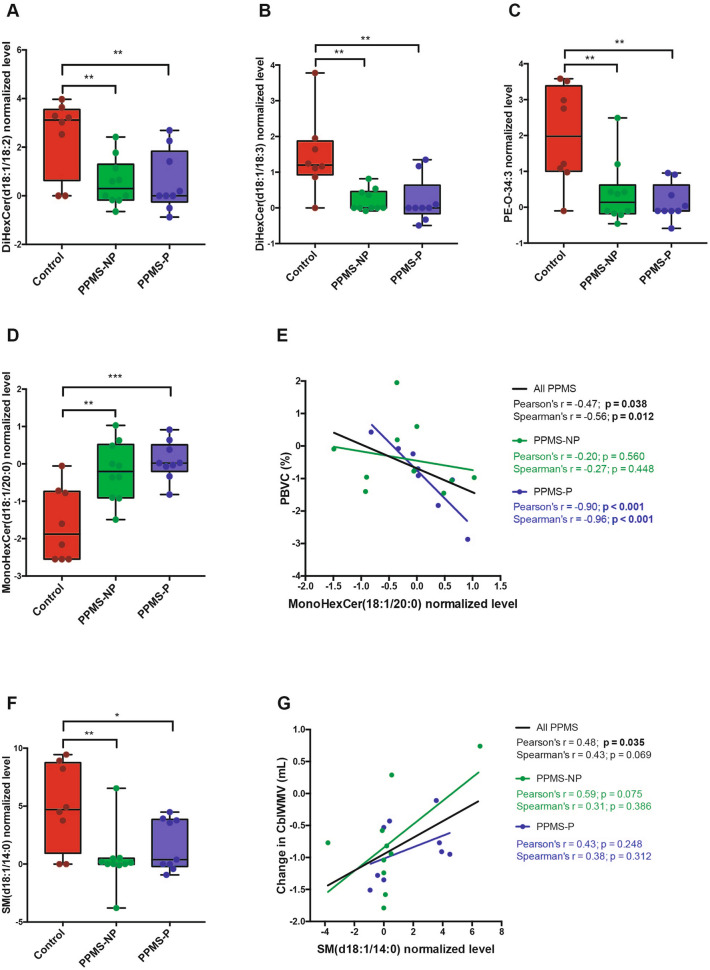
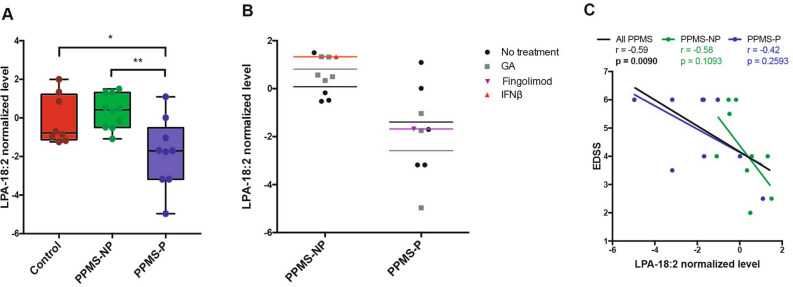
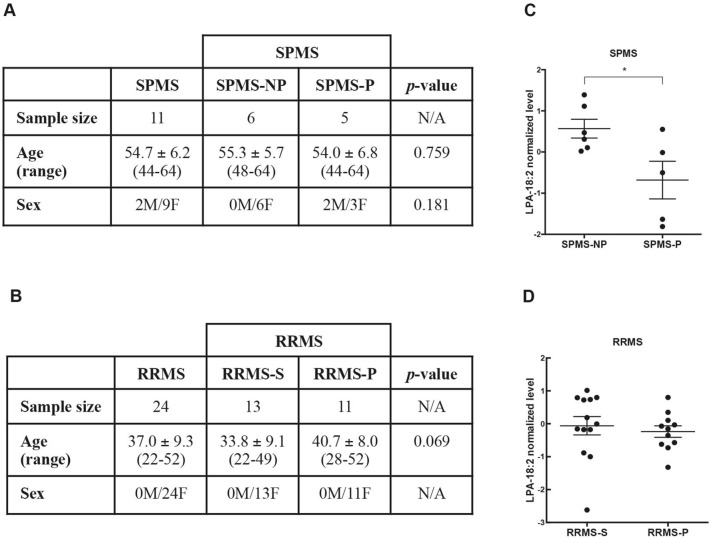
The disease course of patients with a confirmed diagnosis of primary progressive multiple sclerosis (PPMS) is uncertain. In an attempt to identify potential signaling pathways involved in the evolution of the disease, we conducted an exploratory unbiased lipidomic analysis of plasma from non-diseased controls (n = 8) and patients with primary progressive MS (PPMS, n = 19) and either a rapid (PPMS-P, n = 9) or slow (PPMS-NP, n = 10) disease course based on worsening disability and/or MRI-visible appearance of new T2 lesions over a one-year-assessment. Partial least squares-discriminant analysis of the MS/MSALL lipidomic dataset, identified lipids driving the clustering of the groups. Among these lipids, sphingomyelin-d18:1/14:0 and mono-hexosylceramide-d18:1/20:0 were differentially abundant in the plasma of PPMS patients compared to controls and their levels correlated with MRI signs of disease progression. Lyso-phosphatidic acid-18:2 (LPA-18:2) was the only lipid with significantly lower abundance in PPMS patients with a rapidly deteriorating disease course, and its levels inversely correlated with the severity of the neurological deficit. Decreased levels of LPA-18:2 were detected in patients with more rapid disease progression, regardless of therapy and these findings were validated in an independent cohort of secondary progressive (SPMS) patients, but not in a third cohorts of relapsing-remitting (RRMS) patients. Collectively, our analysis suggests that sphingomyelin-d18:1/14:0, mono-hexosylceramide-d18:1/20:0, and LPA-18:2 may represent important targets for future studies aimed at understanding disease progression in MS.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Onset of progressive phase is an age-dependent clinical milestone in multiple sclerosis.Mult Scler. 2013 Feb;19(2):188-98. doi: 10.1177/1352458512451510. Epub 2012 Jun 26. Mult Scler. 2013. PMID: 22736750 Free PMC article.
-
Involvement of cytotoxic Eomes-expressing CD4+ T cells in secondary progressive multiple sclerosis.Proc Natl Acad Sci U S A. 2021 Mar 16;118(11):e2021818118. doi: 10.1073/pnas.2021818118. Proc Natl Acad Sci U S A. 2021. PMID: 33836594 Free PMC article.
-
In vivo evidence of oxidative stress in brains of patients with progressive multiple sclerosis.Mult Scler. 2018 Jul;24(8):1029-1038. doi: 10.1177/1352458517711568. Epub 2017 Jun 1. Mult Scler. 2018. PMID: 28569645 Free PMC article.
-
Mitoxantrone: a review of its use in multiple sclerosis.CNS Drugs. 2004;18(6):379-96. doi: 10.2165/00023210-200418060-00010. CNS Drugs. 2004. PMID: 15089110 Review.
-
A low vitamin D status at diagnosis is associated with an early conversion to secondary progressive multiple sclerosis.J Steroid Biochem Mol Biol. 2016 Nov;164:254-257. doi: 10.1016/j.jsbmb.2015.11.009. Epub 2015 Nov 17. J Steroid Biochem Mol Biol. 2016. PMID: 26598277 Review.
Cited by
-
Myelin Lipid Alterations in Neurodegenerative Diseases: Landscape and Pathogenic Implications.Antioxid Redox Signal. 2024 Dec;41(16-18):1073-1099. doi: 10.1089/ars.2024.0676. Epub 2024 Nov 22. Antioxid Redox Signal. 2024. PMID: 39575748 Review.
-
Recent Advances in Metabolomics and Lipidomics Studies in Human and Animal Models of Multiple Sclerosis.Metabolites. 2024 Oct 13;14(10):545. doi: 10.3390/metabo14100545. Metabolites. 2024. PMID: 39452926 Free PMC article. Review.
-
Plasma Lipidomic Profiling Using Mass Spectrometry for Multiple Sclerosis Diagnosis and Disease Activity Stratification (LipidMS).Int J Mol Sci. 2024 Feb 20;25(5):2483. doi: 10.3390/ijms25052483. Int J Mol Sci. 2024. PMID: 38473733 Free PMC article.
-
Reduced plasma hexosylceramides in frontotemporal dementia are a biomarker of white matter integrity.Alzheimers Dement (Amst). 2025 Jun 4;17(2):e70131. doi: 10.1002/dad2.70131. eCollection 2025 Apr-Jun. Alzheimers Dement (Amst). 2025. PMID: 40469268 Free PMC article.
-
Sphingolipid Players in Multiple Sclerosis: Their Influence on the Initiation and Course of the Disease.Int J Mol Sci. 2022 May 10;23(10):5330. doi: 10.3390/ijms23105330. Int J Mol Sci. 2022. PMID: 35628142 Free PMC article. Review.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
