

Nonpharmacologic Interventions for Reducing Blood Pressure in Adults With Prehypertension to Established Hypertension
- PMID: 32975166
- PMCID: PMC7792371
- DOI: 10.1161/JAHA.120.016804
Nonpharmacologic Interventions for Reducing Blood Pressure in Adults With Prehypertension to Established Hypertension
Abstract
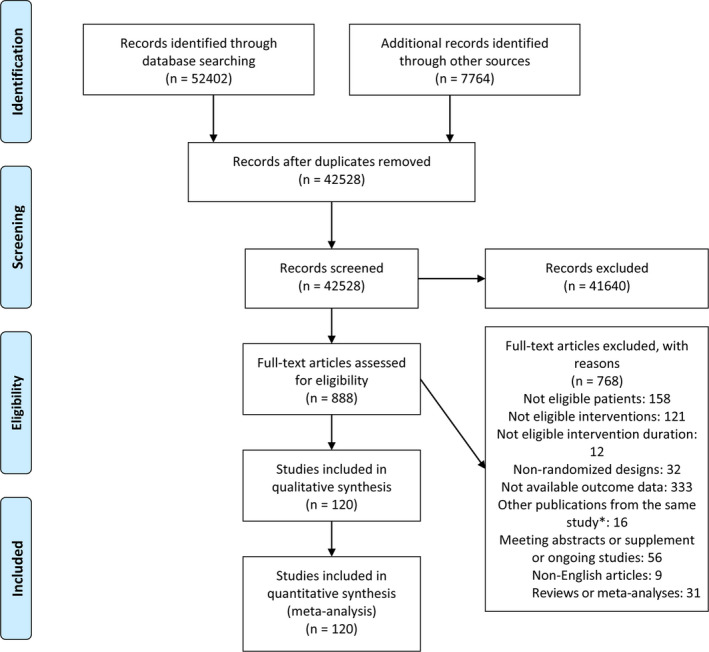
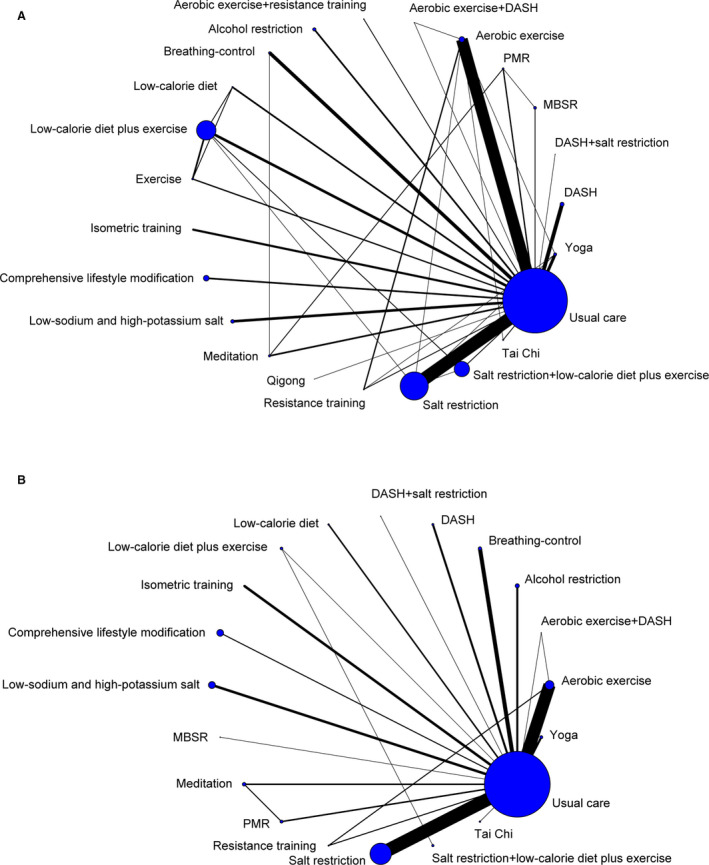
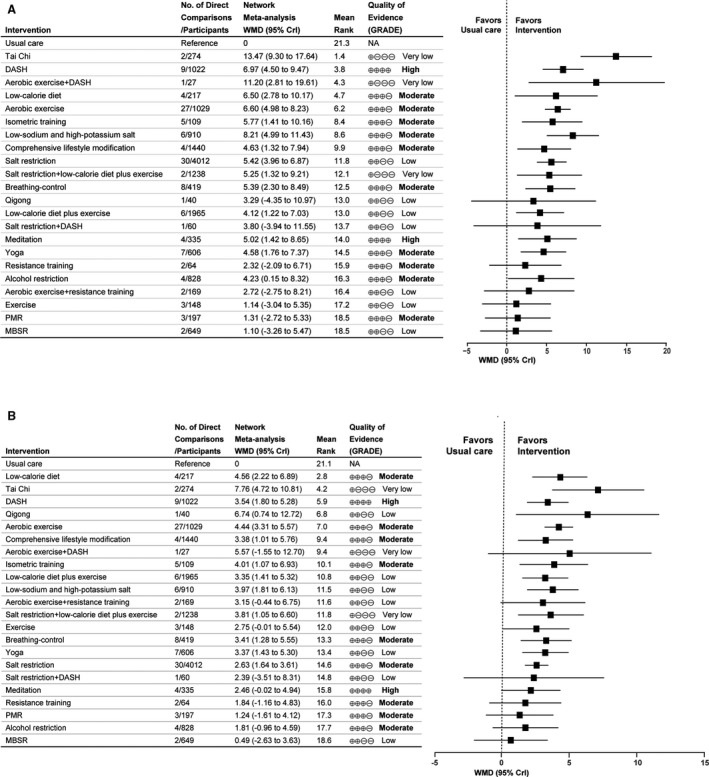
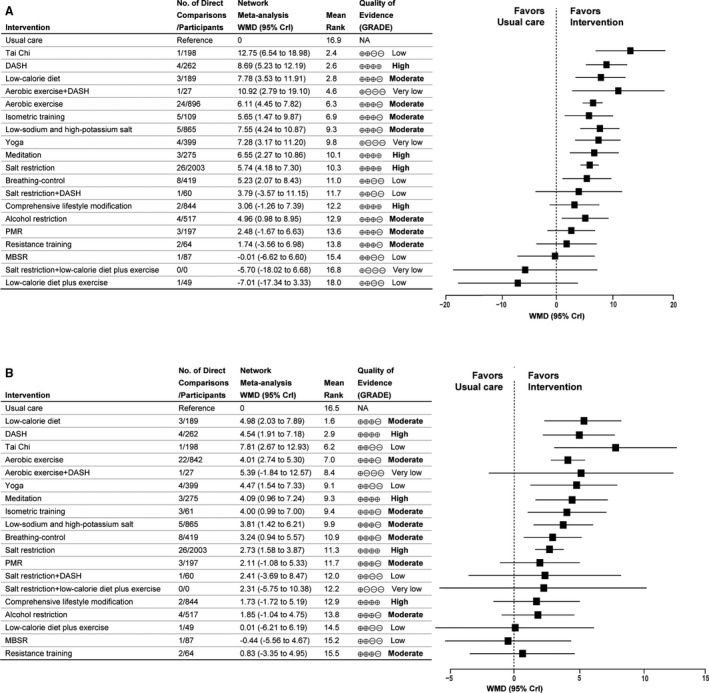
Background Nonpharmacologic interventions that modify lifestyle can lower blood pressure (BP) and have been assessed in numerous randomized controlled trials and pairwise meta-analyses. It is still unclear which intervention would be most efficacious. Methods and Results Bayesian network meta-analyses were performed to estimate the comparative effectiveness of different interventions for lowering BP. From 60 166 potentially relevant articles, 120 eligible articles (14 923 participants) with a median follow-up of 12 weeks, assessing 22 nonpharmacologic interventions, were included. According to the surface under the cumulative ranking probabilities and Grading of Recommendations Assessment, Development and Evaluation (GRADE) quality of evidence, for adults with prehypertension to established hypertension, high-quality evidence indicated that the Dietary Approach to Stop Hypertension (DASH) was superior to usual care and all other nonpharmacologic interventions in lowering systolic BP (weighted mean difference, 6.97 mm Hg; 95% credible interval, 4.50-9.47) and diastolic BP (weighted mean difference, 3.54 mm Hg; 95% credible interval, 1.80-5.28). Compared with usual care, moderate- to high-quality evidence indicated that aerobic exercise, isometric training, low-sodium and high-potassium salt, comprehensive lifestyle modification, breathing-control, and meditation could lower systolic BP and diastolic BP. For patients with hypertension, moderate- to high-quality evidence suggested that the interventions listed (except comprehensive lifestyle modification) were associated with greater systolic BP and diastolic BP reduction than usual care; salt restriction was also effective in lowering both systolic BP and diastolic BP. Among overweight and obese participants, low-calorie diet and low-calorie diet plus exercise could lower more BP than exercise. Conclusions DASH might be the most effective intervention in lowering BP for adults with prehypertension to established hypertension. Aerobic exercise, isometric training, low-sodium and high-potassium salt, comprehensive lifestyle modification, salt restriction, breathing-control, meditation and low-calorie diet also have obvious effects on BP reduction.
Keywords: hypertension; network meta‐analysis; nonpharmacologic interventions; randomized controlled trial; systematic review.
Conflict of interest statement
None.
Figures
References
-
- Lip GYH, Coca A, Kahan T, Boriani G, Manolis AS, Olsen MH, Oto A, Potpara TS, Steffel J, Marín F, et al. Hypertension and cardiac arrhythmias: executive summary of a consensus document from the European Heart Rhythm Association (EHRA) and ESC Council on Hypertension, endorsed by the Heart Rhythm Society (HRS), Asia‐Pacific Heart Rhythm Society (APHRS), and Sociedad Latinoamericana de Estimulación Cardíaca y Electrofisiología (SOLEACE). Eur Heart J Cardiovasc Pharmacother. 2017;235–250. - PubMed
-
- James PA, Oparil S, Carter BL, Cushman WC, Dennison‐Himmelfarb C, Handler J, Lackland DT, LeFevre ML, MacKenzie TD, Ogedegbe O, et al. 2014 evidence‐based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;507–520. - PubMed
-
- Forouzanfar MH, Liu P, Roth GA, Ng M, Biryukov S, Marczak L, Alexander L, Estep K, Hassen Abate K, Akinyemiju TF, et al. Global burden of hypertension and systolic blood pressure of at least 110 to 115 mm Hg, 1990–2015. JAMA. 2017;165–182. - PubMed
-
- Vasan RS, Larson MG, Leip EP, Evans JC, O'Donnell CJ, Kannel WB, Levy D. Impact of high‐normal blood pressure on the risk of cardiovascular disease. N Engl J Med. 2001;1291–1297. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
