

Attributes Germane to Temporomandibular Disorders and Their Associations with Five Chronic Overlapping Pain Conditions
- PMID: 32975541
- PMCID: PMC10073965
- DOI: 10.11607/ofph.2582
Attributes Germane to Temporomandibular Disorders and Their Associations with Five Chronic Overlapping Pain Conditions
Abstract
Aims: To investigate whether TMD-related characteristics are indeed specific to TMD or whether they are also associated with other chronic overlapping pain conditions (COPCs).
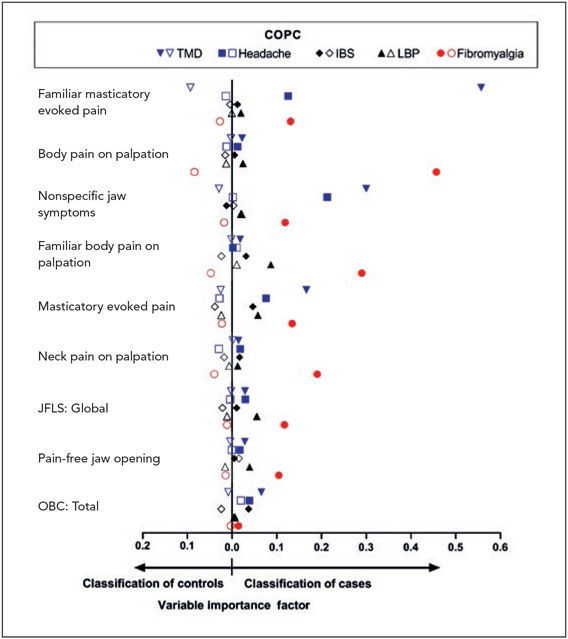
Methods: In this cross-sectional study, 22 characteristics related broadly to TMD (eg, jaw kinesiophobia, overuse behaviors, and functional limitation) were measured in 178 painful TMD cases who were also classified according to four COPCs: headache, low back pain, irritable bowel syndrome, and fibromyalgia. Differences in mean subscale scores were compared according to individual chronic pain conditions and according to number of COPCs.
Results: Headache, low back pain, irritable bowel syndrome, and fibromyalgia were each associated (P < .05) with higher values of at least one TMD-relevant characteristic. In the multivariable analysis, TMD was independently associated with 20 of the 22 characteristics (P < .01), and other COPCs were associated variably. A critical threshold existed between the number of COPCs and TMD characteristics: all characteristics were elevated for subjects with ≥ 3 COPCs (P ≤ .01).
Conclusion: The overlap between COPCs and characteristics typically regarded as specific to painful TMD has implications for treatment targeted at both the local TMD condition and the broader pain disorder underlying the COPC(s). In TMD patients, the overall burden of pain from COPCs may create a shift in the pain-processing systems that underlie these TMD-relevant characteristics.
Figures


Comment in
-
Commentary 3: Temporomandibular Disorders- Casting the Net to Find Answers.J Oral Facial Pain Headache. 2020;34(Suppl):s9-s10. doi: 10.11607/ofph.2020.suppl.c3. J Oral Facial Pain Headache. 2020. PMID: 32975535 No abstract available.
References
-
- Diatchenko L, Nackley AG, Slade GD, Fillingim RB, Maixner W. Idiopathic pain disorders—Pathways of vulnerability. Pain 2006;123:226–230. - PubMed
-
- Yunus MB. Fibromyalgia and overlapping disorders: The unifying concept of central sensitivity syndromes. Semin Arthritis Rheum 2007;36:339–356. - PubMed
-
- Functional pain disorders: Time for a paradigm shift. In: Mayer EA, Bushnell MC (eds). Functional Pain Syndromes: Presentation and Pathophysiology. Seattle: IASP, 2009:531–565.
-
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, ed 3. Cephalalgia 2018;38:1–211. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
