

Exploring How Epidemic Context Influences Syphilis Screening Impact: A Mathematical Modeling Study
- PMID: 32976353
- PMCID: PMC7668348
- DOI: 10.1097/OLQ.0000000000001249
Exploring How Epidemic Context Influences Syphilis Screening Impact: A Mathematical Modeling Study
Abstract
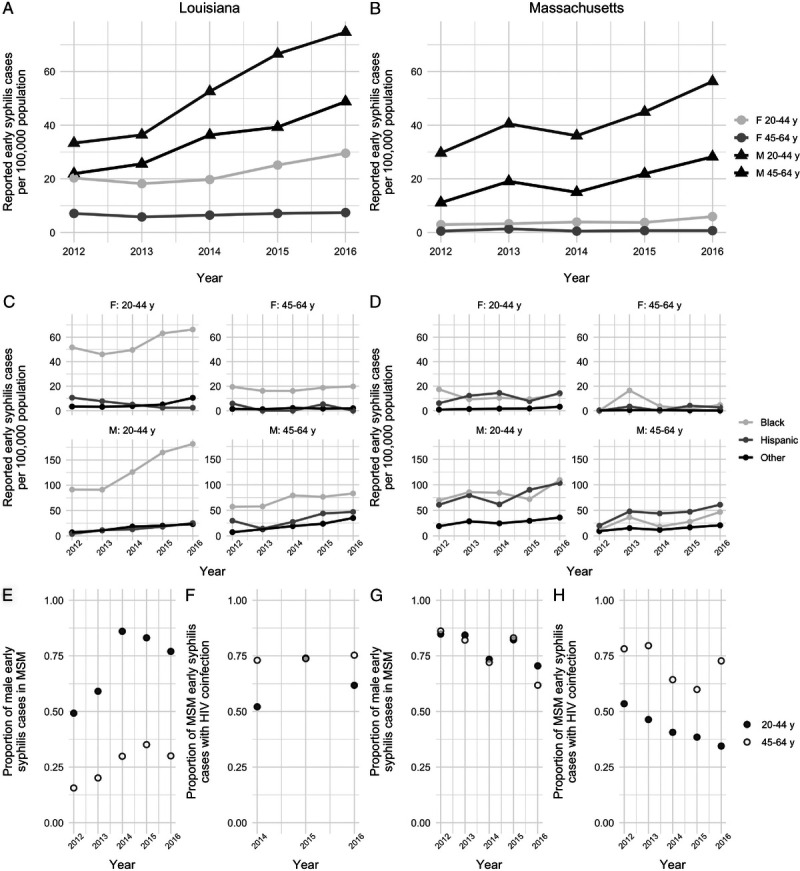
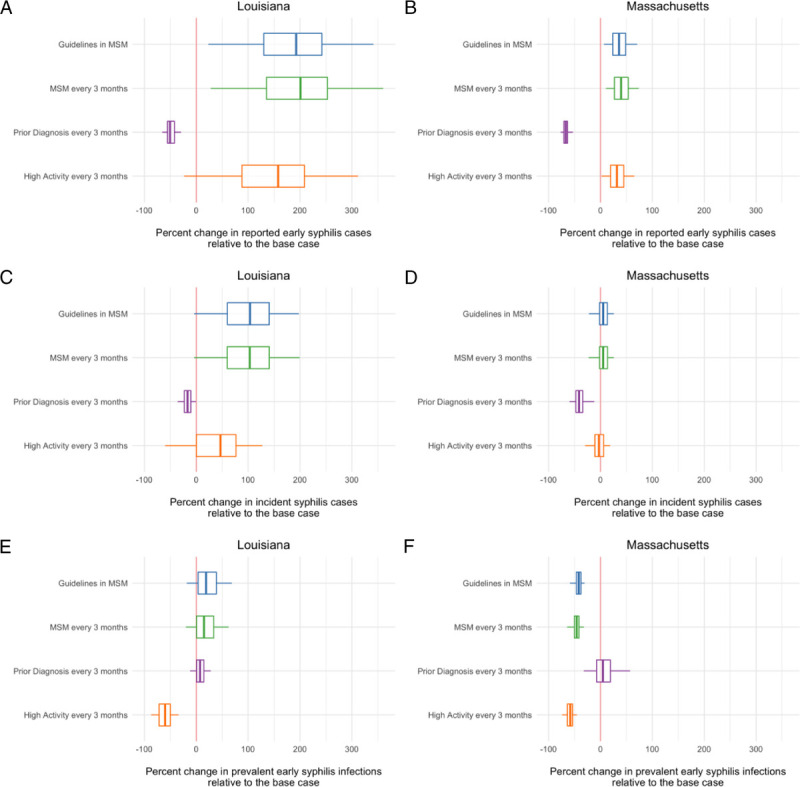
Background: The current syphilis epidemic in the United States is concentrated in gay, bisexual, and other men who have sex with men (MSM), but substantial heterosexual transmission is reported in some parts of the country. Using the US states of Louisiana and Massachusetts as case studies, we investigated how epidemic context influences the impact of population screening approaches for syphilis control.
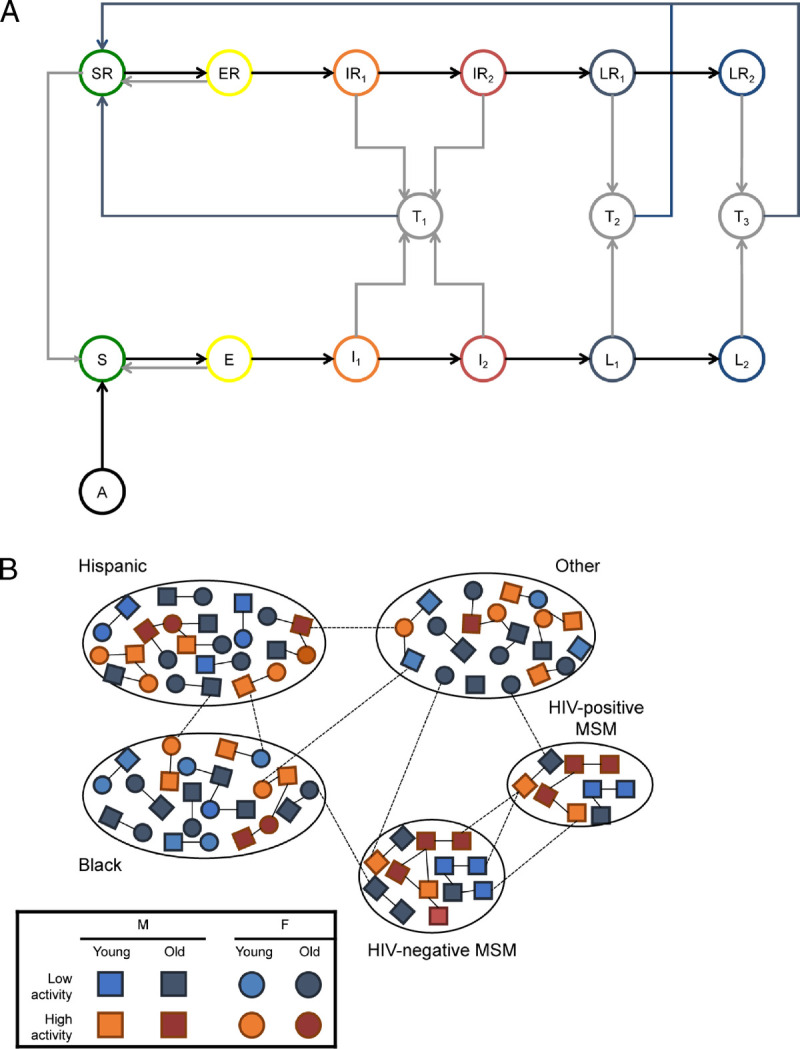
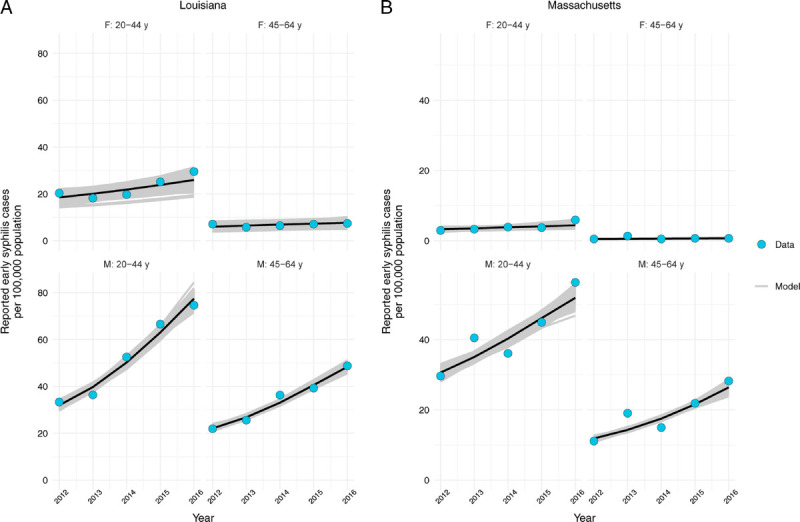
Methods: We constructed a compartmental metapopulation model parameterized to describe observed patterns of syphilis transmission. We estimated the impact of different approaches to screening, including perfect adherence to current US screening guidelines in MSM.
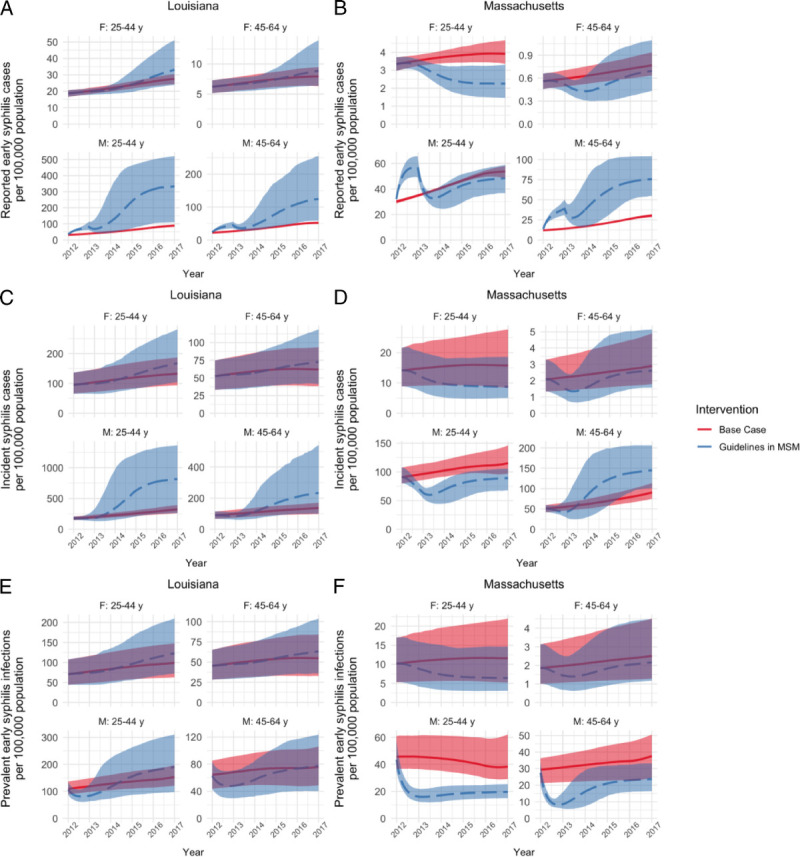
Results: In Louisiana, where syphilis cases are more evenly distributed among MSM and heterosexual populations, we projected that screening according to guidelines would contribute to no change or an increase in syphilis burden, compared with burden with current estimated screening coverage. In Massachusetts, which has a more MSM-focused outbreak, we projected that screening according to guidelines would be as or more effective than current screening coverage in most population groups.
Conclusions: Men who have sex with men-focused approaches to screening may be insufficient for control when there is substantial transmission in heterosexual populations. Epidemic characteristics may be useful when identifying at-risk groups for syphilis screening.
Figures
References
-
- Centers for Disease Control and Prevention. Sexually transmitted disease surveillance 2018. Available at: https://www.cdc.gov/std/stats18/default.htm. 2019. Accessed December 23, 2019.
-
- US Preventive Services Task Force (USPSTF), Bibbins-Domingo K Grossman DC Curry SJ, et al. Screening for syphilis infection in nonpregnant adults and adolescents: US Preventive Services Task Force recommendation statement. JAMA 2016; 315:2321–2327. - PubMed
-
- US Preventive Services Task Force, Curry SJ Krist AH Owens DK, et al. Screening for syphilis infection in pregnant women: US Preventive Services Task Force reaffirmation recommendation statement. JAMA 2018; 320:911–917. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
