

Temporal Clusters of Kawasaki Disease Cases Share Distinct Phenotypes That Suggest Response to Diverse Triggers
- PMID: 32976897
- PMCID: PMC7506475
- DOI: 10.1016/j.jpeds.2020.09.043
Temporal Clusters of Kawasaki Disease Cases Share Distinct Phenotypes That Suggest Response to Diverse Triggers
Abstract
Objective: To test the hypothesis that cases of Kawasaki disease within a temporal cluster have a similar pattern of host response that is distinct from cases of Kawasaki disease in different observed clusters and randomly constructed clusters.
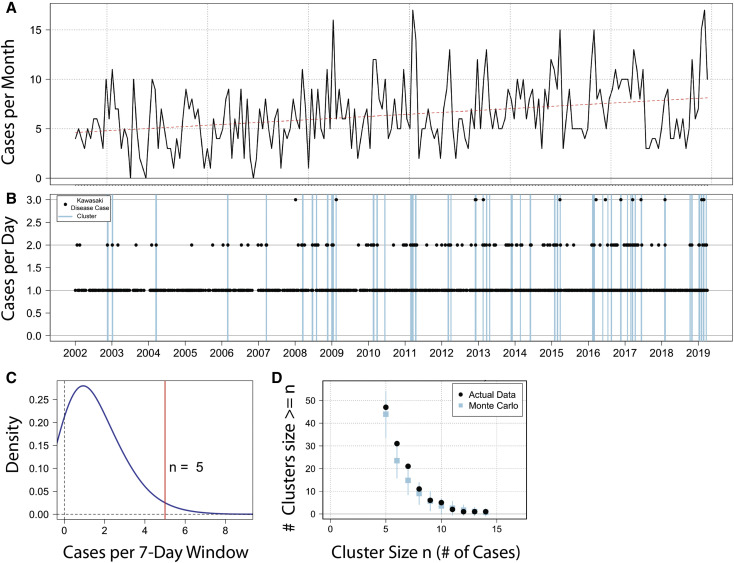
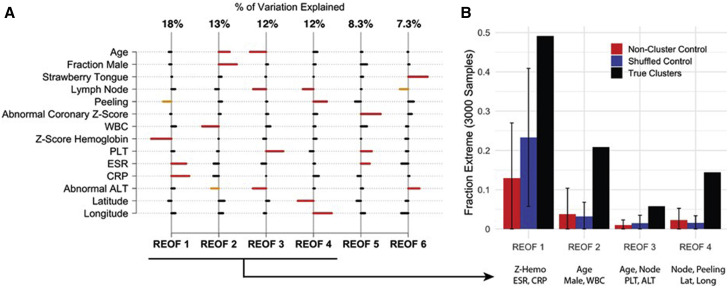
Study design: We designed a case-control study to analyze 47 clusters derived from 1332 patients with Kawasaki disease over a 17-year period (2002-2019) from a single clinical site and compared the cluster characteristics with those of 2 control groups of synthetic Kawasaki disease clusters. We defined a "true" Kawasaki disease cluster as at least 5 patients within a 7-day moving window. The observed and synthetic Kawasaki disease clusters were compared with respect to demographic and clinical characteristics and median values for standard laboratory data using univariate analysis and a multivariate, rotated empirical orthogonal function analysis.
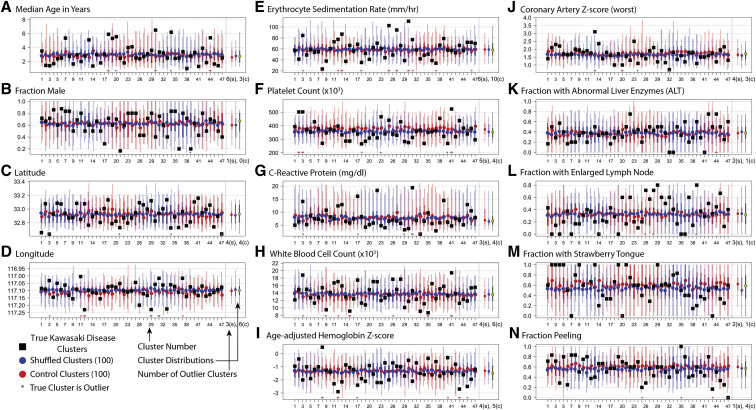
Results: In a univariate analysis, the median values for age, coronary artery z-score, white blood cell count, erythrocyte sedimentation rate, C-reactive protein, and age-adjusted hemoglobin for several of the true Kawasaki disease clusters exceeded the 95th percentile for the 2 synthetic clusters. REOF analyses revealed distinct patterns of demographic and clinical measures within clusters.
Conclusions: Cases of Kawasaki disease within a cluster were more similar with respect to demographic and clinical features and levels of inflammation than would be expected by chance. These observations suggest that different triggers and/or different intensities of exposures result in clusters of cases of Kawasaki disease that share a similar response pattern. Analyzing cases within clusters or cases who share demographic and clinical features may lead to new insights into the etiology of Kawasaki disease.
Keywords: coronary artery aneurysm; epidemiology; pediatrics; vasculitis.
Copyright © 2020 Elsevier Inc. All rights reserved.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
