

Comparison of Patch Materials for Pulmonary Artery Reconstruction
- PMID: 32977008
- PMCID: PMC7985045
- DOI: 10.1053/j.semtcvs.2020.09.011
Comparison of Patch Materials for Pulmonary Artery Reconstruction
Abstract
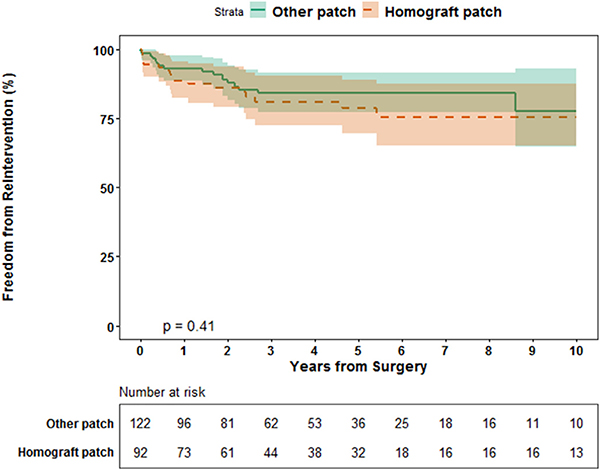
Various patch materials with variable cost are used for pulmonary artery reconstruction. An analysis of reintervention based on type of patch material might inform value-based decision making. This was a retrospective review of 214 sites of pulmonary artery reconstruction at a single center from 2000 to 2014. We excluded patients with unifocalization of aortopulmonary collaterals. Primary outcome was reintervention for each type of patch. Total number of patch sites was 214 (180 patients). Median follow-up was 3.7 years. Patch materials and number of sites were branch patch homograft (92), bovine pericardium (44), autologous pericardium (41), and porcine intestinal submucosal patch (37). Median age and weight at the time of patch reconstruction were 12.1 months and 8.5 kg. Reintervention occurred at 34 sites (15.9%). With Cox proportional hazards regression, the following variables were associated with reinterevention: preoperative renal failure - hazard ratio of 4.36 (1.87-10.16), P < 0.001 and weight at surgery - hazard ratio 0.93 (0.89-0.98), P = 0.004. Patch type was not related to reintervention (P = 0.197). Cost per unit patch ranged from $0 (dollars, US) for untreated autologous pericardium to $6,105 for homograft branch patch. In this retrospective analysis, there was no relationship between type of patch used for main or central branch pulmonary artery reconstruction and subsequent reintervention on that site. This finding, combined with the widely disparate costs of patches, may help inform value-based decision making.
Keywords: Patch; Pulmonary artery; Reconstruction; Reintervention.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosures: Michael E Mitchell, MD is co-founder of Ariosa Diagnostics and TAI Diagnostics. Neither are related to the content of this manuscript. Ronald K. Woods, MD, PhD is co-founder of OperVu, Inc. with no relationship to the content of this work. All other authors have no disclosures or potential conflict of interest.
Figures



Comment in
-
Commentary: A Plentiful Patchwork for Patching Pulmonary Arteries.Semin Thorac Cardiovasc Surg. 2021 Summer;33(2):467-468. doi: 10.1053/j.semtcvs.2020.10.010. Epub 2020 Nov 7. Semin Thorac Cardiovasc Surg. 2021. PMID: 33171238 No abstract available.
-
Commentary: Cost of Doing Business.Semin Thorac Cardiovasc Surg. 2021 Summer;33(2):466. doi: 10.1053/j.semtcvs.2020.10.011. Epub 2020 Nov 7. Semin Thorac Cardiovasc Surg. 2021. PMID: 33171240 No abstract available.
References
-
- Cresalia NM, Armstrong AK, Romano JC, et al.: Long-term outcomes after surgical pulmonary arterioplasty and risk factors for reintervention. Ann Thorac Surg 105:622–628, 2018 - PubMed
-
- Fraint HY, Richmond ME, Bacha EA, et al.: Comparison of extracellular matrix patch and standard patch material in the pulmonary arteries. Pediatr Cardiol 37:1162–1168, 2016 - PubMed
-
- Hopkins RA, Lofland GF, Marshall J, et al.: Pulmonary arterioplasty with decellularized allogenic patches. Ann Thorac Surg 97:1407–1413, 2014 - PubMed
-
- Hawkins JA, Breinholt JP, Lambert LM, et al.: Class I and class II anti-hla antibodies after implantation of cryopreserved allograft material in pediatric patients. J Thorac Cardiovasc Surg 119:324–330, 2000 - PubMed
-
- Hawkins JA, Hillman ND, Lambert LM, et al.: Immunogenicity of decelluralized cryoprerved allografts in pediatric cardiac surgery: comparison with standard cryopreserved allografts. J Thorac Cardiovasc Surg 126:247–253, 2003 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
