

Technology-aided assessment of functionally relevant sensorimotor impairments in arm and hand of post-stroke individuals
- PMID: 32977810
- PMCID: PMC7517659
- DOI: 10.1186/s12984-020-00748-5
Technology-aided assessment of functionally relevant sensorimotor impairments in arm and hand of post-stroke individuals
Abstract
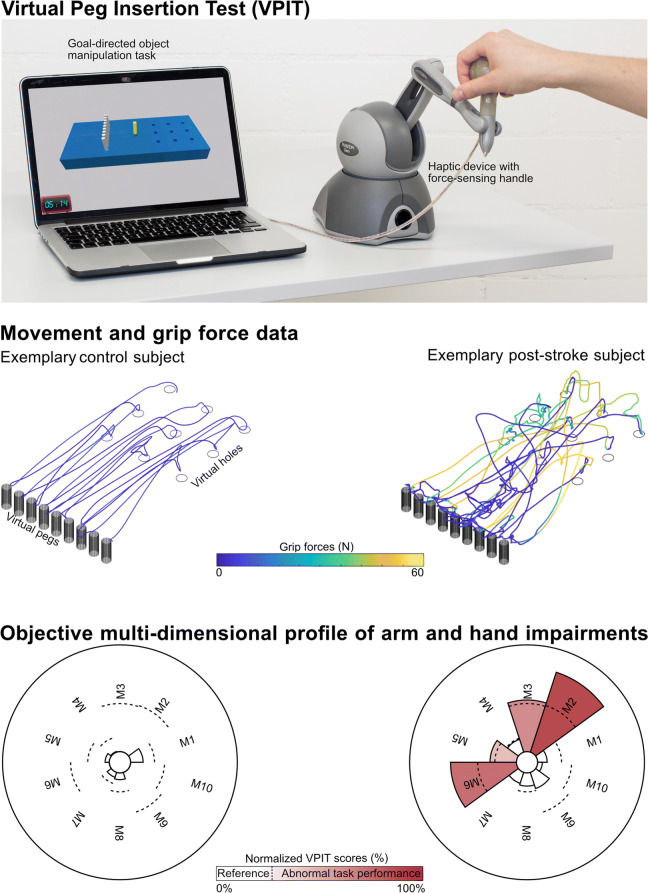
Background: Assessing arm and hand sensorimotor impairments that are functionally relevant is essential to optimize the impact of neurorehabilitation interventions. Technology-aided assessments should provide a sensitive and objective characterization of upper limb impairments, but often provide arm weight support and neglect the importance of the hand, thereby questioning their functional relevance. The Virtual Peg Insertion Test (VPIT) addresses these limitations by quantifying arm and hand movements as well as grip forces during a goal-directed manipulation task requiring active lifting of the upper limb against gravity. The aim of this work was to evaluate the ability of the VPIT metrics to characterize arm and hand sensorimotor impairments that are relevant for performing functional tasks.
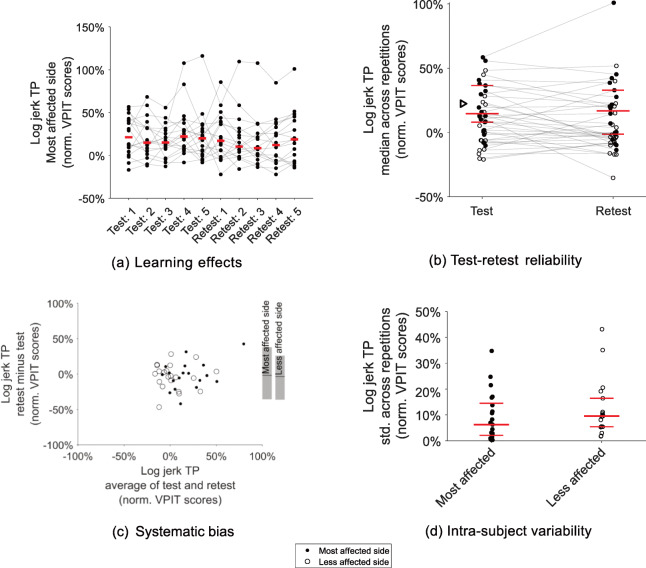
Methods: Arm and hand sensorimotor impairments were systematically characterized in 30 chronic stroke patients using conventional clinical scales and the VPIT. For the latter, ten previously established kinematic and kinetic core metrics were extracted. The validity and robustness of these metrics was investigated by analyzing their clinimetric properties (test-retest reliability, measurement error, learning effects, concurrent validity).
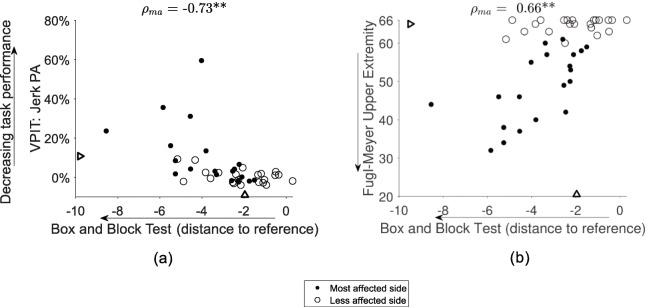
Results: Twenty-three of the participants, the ones with mild to moderate sensorimotor impairments and without strong cognitive deficits, were able to successfully complete the VPIT protocol (duration 16.6 min). The VPIT metrics detected impairments in arm and hand in 90.0% of the participants, and were sensitive to increased muscle tone and pathological joint coupling. Most importantly, significant moderate to high correlations between conventional scales of activity limitations and the VPIT metrics were found, thereby indicating their functional relevance when grasping and transporting objects, and when performing dexterous finger manipulations. Lastly, the robustness of three out of the ten VPIT core metrics in post-stroke individuals was confirmed.
Conclusions: This work provides evidence that technology-aided assessments requiring goal-directed manipulations without arm weight support can provide an objective, robust, and clinically feasible way to assess functionally relevant sensorimotor impairments in arm and hand in chronic post-stroke individuals with mild to moderate deficits. This allows for a better identification of impairments with high functional relevance and can contribute to optimizing the functional benefits of neurorehabilitation interventions.
Keywords: Digital health metrics; Motor control; Neurological disorders; Upper limb assessment.
Conflict of interest statement
Andreas R. Luft is a scientific advisor to Hocoma AG (Volketswil, Switzerland). The remaining authors have no conflict of interest in the submission of this manuscript.
Figures
Similar articles
-
Influence of virtual reality and task complexity on digital health metrics assessing upper limb function.J Neuroeng Rehabil. 2024 Jul 27;21(1):125. doi: 10.1186/s12984-024-01413-x. J Neuroeng Rehabil. 2024. PMID: 39068424 Free PMC article.
-
Concurrent validity and test-retest reliability of the Virtual Peg Insertion Test to quantify upper limb function in patients with chronic stroke.J Neuroeng Rehabil. 2016 Jan 22;13:8. doi: 10.1186/s12984-016-0116-y. J Neuroeng Rehabil. 2016. PMID: 26801395 Free PMC article.
-
Reliability and validity of digital health metrics for assessing arm and hand impairments in an ataxic disorder.Ann Clin Transl Neurol. 2022 Apr;9(4):432-443. doi: 10.1002/acn3.51493. Epub 2022 Feb 27. Ann Clin Transl Neurol. 2022. PMID: 35224896 Free PMC article.
-
Systematic Review on Kinematic Assessments of Upper Limb Movements After Stroke.Stroke. 2019 Mar;50(3):718-727. doi: 10.1161/STROKEAHA.118.023531. Stroke. 2019. PMID: 30776997
-
Quantitative assessment based on kinematic measures of functional impairments during upper extremity movements: A review.Clin Biomech (Bristol). 2014 Aug;29(7):719-27. doi: 10.1016/j.clinbiomech.2014.06.013. Epub 2014 Jun 26. Clin Biomech (Bristol). 2014. PMID: 25017296 Review.
Cited by
-
Arm impairment and walking speed explain real-life activity of the affected arm and leg after stroke.J Rehabil Med. 2021 Jun 23;53(6):jrm00210. doi: 10.2340/16501977-2838. J Rehabil Med. 2021. PMID: 33948673 Free PMC article.
-
Personalized prediction of rehabilitation outcomes in multiple sclerosis: a proof-of-concept using clinical data, digital health metrics, and machine learning.Med Biol Eng Comput. 2022 Jan;60(1):249-261. doi: 10.1007/s11517-021-02467-y. Epub 2021 Nov 25. Med Biol Eng Comput. 2022. PMID: 34822120 Free PMC article.
-
U-Limb: A multi-modal, multi-center database on arm motion control in healthy and post-stroke conditions.Gigascience. 2021 Jun 18;10(6):giab043. doi: 10.1093/gigascience/giab043. Gigascience. 2021. PMID: 34143875 Free PMC article.
-
Enhancing Hand Sensorimotor Function in Individuals with Cervical Spinal Cord Injury: A Novel Tactile Discrimination Feedback Approach Using a Multiple-Baseline Design.Brain Sci. 2025 Mar 28;15(4):352. doi: 10.3390/brainsci15040352. Brain Sci. 2025. PMID: 40309804 Free PMC article.
-
Influence of virtual reality and task complexity on digital health metrics assessing upper limb function.J Neuroeng Rehabil. 2024 Jul 27;21(1):125. doi: 10.1186/s12984-024-01413-x. J Neuroeng Rehabil. 2024. PMID: 39068424 Free PMC article.
References
-
- Benjamin EJ, Muntner P, Alonso A, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Chang AR, Cheng S, Das SR, Delling FN, Djousse L, Elkind MSV, Ferguson JF, Fornage M, Jordan LC, Khan SS, Kissela BM, Knutson KL, Kwan TW, Lackland DT, Lewis TT, Lichtman JH, Longenecker CT, Loop MS, Lutsey PL, Martin SS, Matsushita K, Moran AE, Mussolino ME, O’Flaherty M, Pandey A, Perak AM, Rosamond WD, Roth GA, Sampson UKA, Satou GM, Schroeder EB, Shah SH, Spartano NL, Stokes A, Tirschwell DL, Tsao CW, Turakhia MP, VanWagner LB, Wilkins JT, Wong SS, Virani SS. Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association. Am Heart Assoc. 2019;139(10):e56–e528. - PubMed
-
- World Health Organization. International classification of functioning, disability and health: ICF. World Health Organ. 2001. 10.4135/9781412950510.n454.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
