

The use of both internal thoracic arteries for coronary revascularization increases the estimate of post-operative lower limb ischemia in patients with peripheral artery disease
- PMID: 32977844
- PMCID: PMC7519572
- DOI: 10.1186/s13019-020-01315-8
The use of both internal thoracic arteries for coronary revascularization increases the estimate of post-operative lower limb ischemia in patients with peripheral artery disease
Abstract
Background: Patients with a history of peripheral arterial disease (PAD) undergoing coronary artery bypass grafting (CABG) exhibit higher rates of complications. There are conflicting data on the survival benefits for bilateral thoracic artery (BITA) grafting compared with left internal thoracic artery (LITA) CABG in patients with PAD. The aim of the study was to explore the influence of the use of BITA grafts vs. LITA for CABG on post-operative acute lower limb ischemia (ALLI) and main post-operative complications in patients with concomitant PAD.
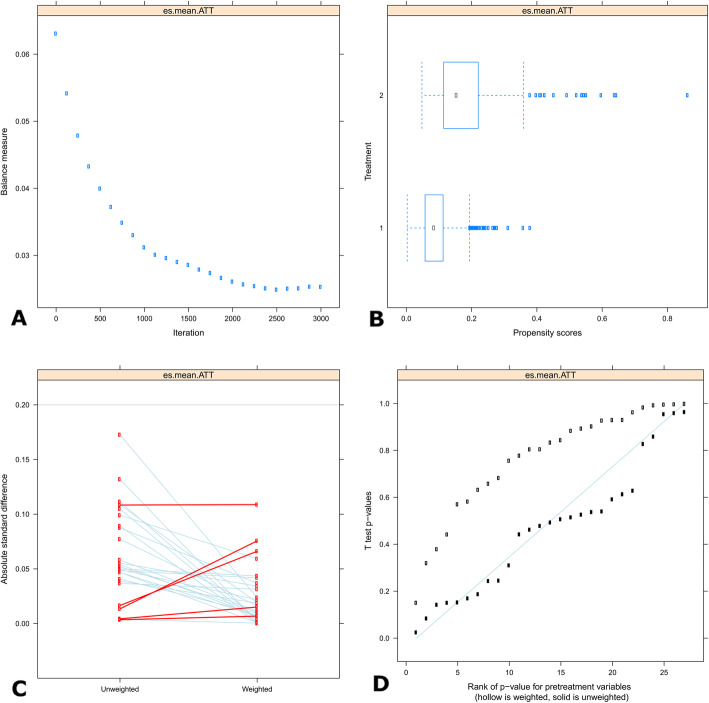
Methods: We used a propensity-score (PS) based analysis to compare outcomes between the two surgical procedures, BITA and LITA. The inverse probability of treatment weighting PS technique was applied to adjust for pre- and intra-operative confounders, and to get optimal balancing of the pre-operative data. The primary outcome was the estimate of postoperative ALLI. Secondary outcomes included overall death and death of cardiac causes within 30 days of surgery, stroke and acute kidney disease (AKD).
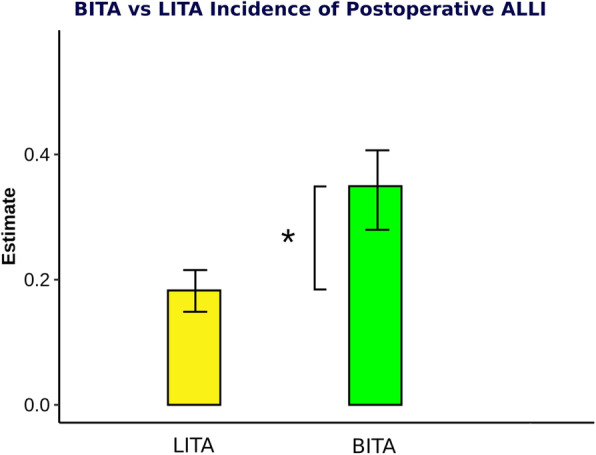
Results: The study population consisted of 1961 patients. The LITA procedure was performed in 1768 patients whereas 193 patients underwent a BITA technique. The estimate of ALLI was 14% higher in the BITA compared to the LITA (p < 0.001) group. Thirty-day mortality, cardiac death, occurrence of stroke and AKI did not differ significantly between the groups.
Conclusions: The use of both ITAs led to a significant increase in ALLI. This result was most likely caused by the complete disruption of the ITA collateral providing additional blood supply to the lower extremities. Based on our data, BITA should be used with extreme caution in PAD patients. Further research on this topic is necessary to confirm our findings.
Keywords: Coronary disease; Limb ischemia; Peripheral artery disease.
Conflict of interest statement
None to be disclosed.
Figures
Similar articles
-
Outcomes following surgical revascularization with single versus bilateral internal thoracic arterial grafts in patients with left main coronary artery disease undergoing coronary artery bypass grafting: insights from the EXCEL trial†.Eur J Cardiothorac Surg. 2019 Mar 1;55(3):501-510. doi: 10.1093/ejcts/ezy291. Eur J Cardiothorac Surg. 2019. PMID: 30165487 Clinical Trial.
-
Early outcomes following isolated coronary artery bypass surgery: Influence of peripheral artery disease.J Card Surg. 2019 Dec;34(12):1470-1477. doi: 10.1111/jocs.14263. Epub 2019 Sep 19. J Card Surg. 2019. PMID: 31536148
-
Long-term Outcomes of Multiple Arterial Coronary Artery Bypass Grafting: A Population-Based Study of Patients in British Columbia, Canada.JAMA Cardiol. 2017 Nov 1;2(11):1187-1196. doi: 10.1001/jamacardio.2017.3705. JAMA Cardiol. 2017. PMID: 29049458 Free PMC article.
-
Use Rate and Outcome in Bilateral Internal Thoracic Artery Grafting: Insights From a Systematic Review and Meta-Analysis.J Am Heart Assoc. 2018 May 17;7(11):e009361. doi: 10.1161/JAHA.118.009361. J Am Heart Assoc. 2018. PMID: 29773579 Free PMC article.
-
Bilateral internal thoracic artery harvest and deep sternal wound infection in diabetic patients.Ann Thorac Surg. 2013 Mar;95(3):862-9. doi: 10.1016/j.athoracsur.2012.11.068. Epub 2013 Jan 24. Ann Thorac Surg. 2013. PMID: 23352296 Review.
Cited by
-
Deep inferior epigastric artery as a collateral pathway to the lower extremities: A case report.JPRAS Open. 2022 Jan 23;32:13-17. doi: 10.1016/j.jpra.2022.01.003. eCollection 2022 Jun. JPRAS Open. 2022. PMID: 35242983 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
