

Left ventricular longitudinal shortening: relation to stroke volume and ejection fraction in ageing, blood pressure, body size and gender in the HUNT3 study
- PMID: 32978265
- PMCID: PMC7520903
- DOI: 10.1136/openhrt-2020-001243
Left ventricular longitudinal shortening: relation to stroke volume and ejection fraction in ageing, blood pressure, body size and gender in the HUNT3 study
Abstract
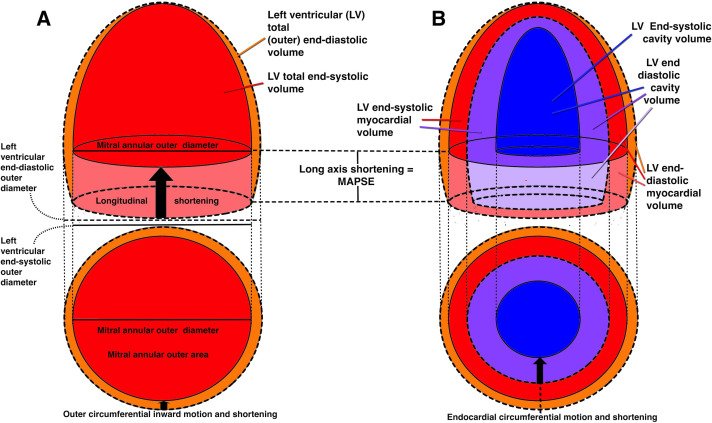
Background: Aims of this cross-sectional study were to assess: the relative contribution of left ventricular (LV) systolic long-axis shortening (mean mitral annular plane systolic excursion, MAPSE) to stroke volume (SV), the mechanisms for preserved ejection fraction (EF) despite reduced MAPSE, the age dependency of myocardial volume and myocardial systolic compression.
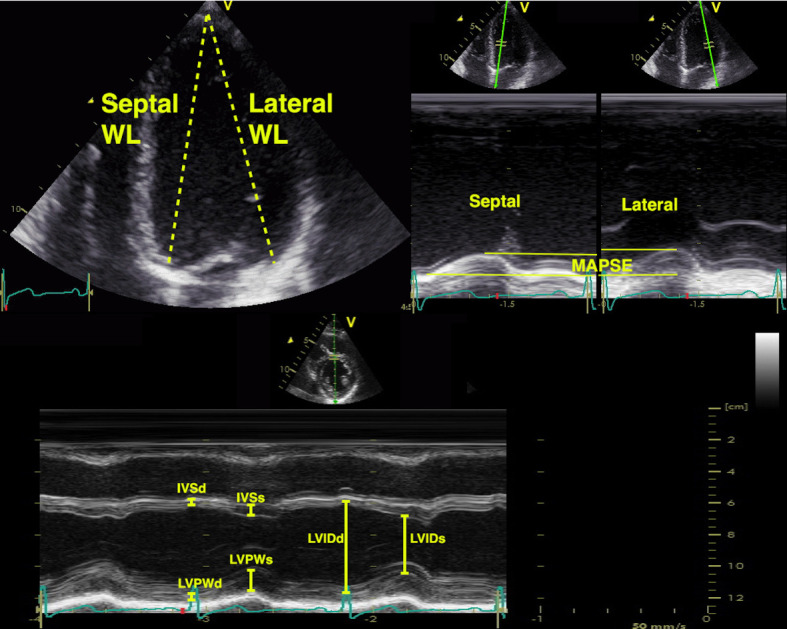
Methods: Linear dimensions and longitudinal and cross-sectional M-modes were acquired in 1266 individuals without history of heart disease, diabetes or known hypertension from the third wave of the Nord-Trøndelag Health Study. Measurements were entered into a half-ellipsoid LV model for volume calculations, and volumes were related to age, body size (body surface area, BSA), sex and blood pressure (BP).
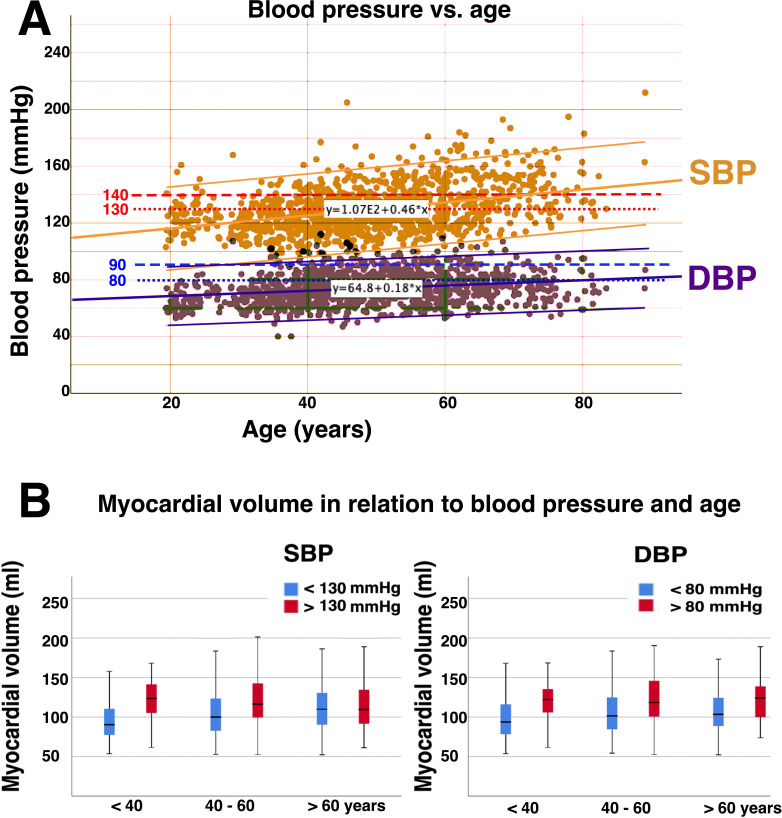
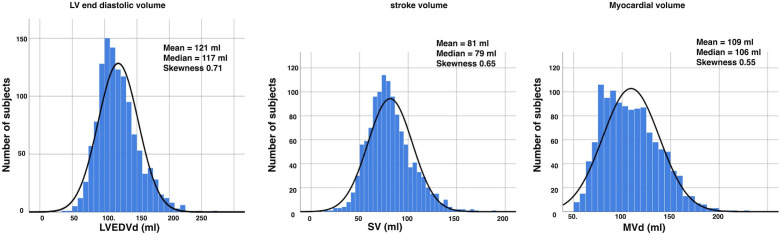
Results: Mean BP and proportion with hypertensive values increased with increasing age. MAPSE contributed to 75% of SV, with no relation to age or BSA as both MAPSE and SV decreased with increasing age. LV end-diastolic volume (LVEDV) and SV increased with BSA and decreased with higher age; EF was not related to age or BSA. Myocardial volume increased with higher age and BSA, with an additional gender dependency. The association of age with myocardial volume was not significant when corrected for BP, while both systolic and diastolic BP were significant associated with myocardial volume. Myocardial compression was less than 3%.
Conclusions: MAPSE contributes approximately 75% and short axis shortening 25% to SV. Both decline with age, but their percentage contributions to SV are unchanged. EF is preserved by the simultaneous decrease in LVEDV and SV. Myocardial volume is positively associated with age, but this is only related to higher BP, which may have implications for BP treatment in ageing. The myocardium is near incompressible.
Keywords: cardiac function; echocardiography; hypertension.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Relation between Mitral Annular Plane Systolic Excursion and Global longitudinal strain in normal subjects: The HUNT study.Echocardiography. 2018 May;35(5):603-610. doi: 10.1111/echo.13825. Epub 2018 Feb 4. Echocardiography. 2018. PMID: 29399886
-
Mitral annular plane systolic excursion/left ventricular length (MAPSE/L) as a simple index for assessing left ventricular longitudinal function in children.Echocardiography. 2016 Nov;33(11):1703-1709. doi: 10.1111/echo.13325. Epub 2016 Aug 22. Echocardiography. 2016. PMID: 27545275
-
Ethnic-Specific Normative Reference Values for Echocardiographic LA and LV Size, LV Mass, and Systolic Function: The EchoNoRMAL Study.JACC Cardiovasc Imaging. 2015 Jun;8(6):656-65. doi: 10.1016/j.jcmg.2015.02.014. Epub 2015 May 14. JACC Cardiovasc Imaging. 2015. PMID: 25981507
-
Clinical implication of mitral annular plane systolic excursion for patients with cardiovascular disease.Eur Heart J Cardiovasc Imaging. 2013 Mar;14(3):205-12. doi: 10.1093/ehjci/jes240. Epub 2012 Nov 15. Eur Heart J Cardiovasc Imaging. 2013. PMID: 23161791 Review.
-
Changes in left ventricular size, geometry, pump function and left heart pressures during healthy aging.Rev Cardiovasc Med. 2021 Sep 24;22(3):717-729. doi: 10.31083/j.rcm2203079. Rev Cardiovasc Med. 2021. PMID: 34565071 Review.
Cited by
-
Sex-specific differences in left ventricular mass and myocardial energetic efficiency in non-diabetic, pre-diabetic and newly diagnosed type 2 diabetic subjects.Cardiovasc Diabetol. 2021 Mar 6;20(1):60. doi: 10.1186/s12933-021-01248-z. Cardiovasc Diabetol. 2021. PMID: 33676510 Free PMC article.
-
Global longitudinal strain is an informative index of left ventricular performance in neonates receiving intensive care.Sci Rep. 2024 Apr 17;14(1):8881. doi: 10.1038/s41598-024-59441-5. Sci Rep. 2024. PMID: 38632330 Free PMC article.
-
Correlation between tissue Doppler-derived left ventricular systolic velocity (S') and left ventricle ejection fraction in sepsis and septic shock: a retrospective cohort study.J Intensive Care. 2023 Jul 3;11(1):28. doi: 10.1186/s40560-023-00678-z. J Intensive Care. 2023. PMID: 37400918 Free PMC article.
-
Sex Differences in Molecular Mechanisms of Cardiovascular Aging.Front Aging. 2021 Sep 10;2:725884. doi: 10.3389/fragi.2021.725884. eCollection 2021. Front Aging. 2021. PMID: 35822017 Free PMC article. Review.
-
Myocardial deformation imaging by 2D speckle tracking echocardiography for assessment of diastolic dysfunction in murine cardiopathology.Sci Rep. 2023 Jul 31;13(1):12344. doi: 10.1038/s41598-023-39499-3. Sci Rep. 2023. PMID: 37524893 Free PMC article.
References
-
- Lundbäck S. Cardiac pumping and function of the ventricular septum. Acta Physiol Scand Suppl 1986;550:1–101. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources