

Systematic evaluation and external validation of 22 prognostic models among hospitalised adults with COVID-19: an observational cohort study
- PMID: 32978307
- PMCID: PMC7518075
- DOI: 10.1183/13993003.03498-2020
Systematic evaluation and external validation of 22 prognostic models among hospitalised adults with COVID-19: an observational cohort study
Abstract
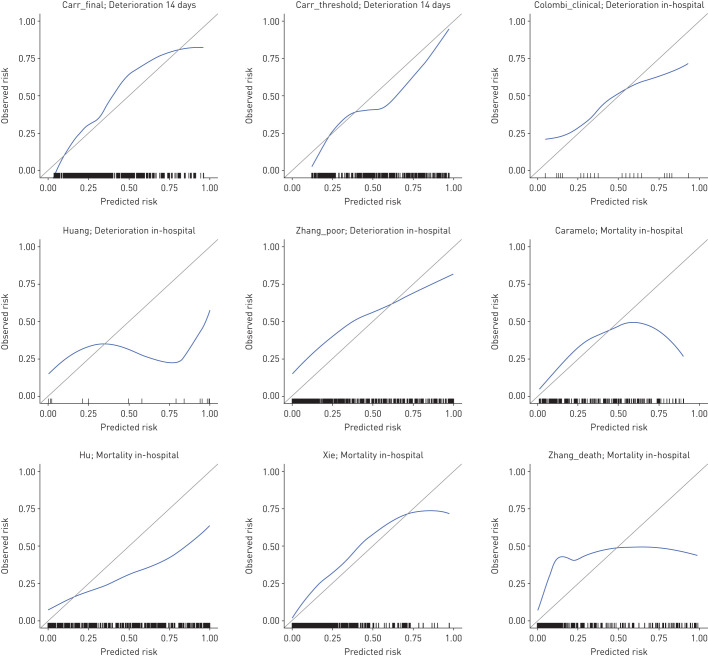
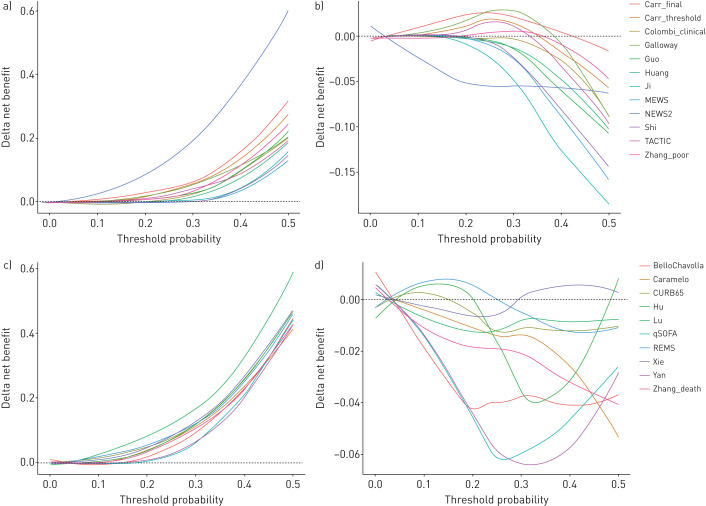
The number of proposed prognostic models for coronavirus disease 2019 (COVID-19) is growing rapidly, but it is unknown whether any are suitable for widespread clinical implementation.We independently externally validated the performance of candidate prognostic models, identified through a living systematic review, among consecutive adults admitted to hospital with a final diagnosis of COVID-19. We reconstructed candidate models as per original descriptions and evaluated performance for their original intended outcomes using predictors measured at the time of admission. We assessed discrimination, calibration and net benefit, compared to the default strategies of treating all and no patients, and against the most discriminating predictors in univariable analyses.We tested 22 candidate prognostic models among 411 participants with COVID-19, of whom 180 (43.8%) and 115 (28.0%) met the endpoints of clinical deterioration and mortality, respectively. Highest areas under receiver operating characteristic (AUROC) curves were achieved by the NEWS2 score for prediction of deterioration over 24 h (0.78, 95% CI 0.73-0.83), and a novel model for prediction of deterioration <14 days from admission (0.78, 95% CI 0.74-0.82). The most discriminating univariable predictors were admission oxygen saturation on room air for in-hospital deterioration (AUROC 0.76, 95% CI 0.71-0.81), and age for in-hospital mortality (AUROC 0.76, 95% CI 0.71-0.81). No prognostic model demonstrated consistently higher net benefit than these univariable predictors, across a range of threshold probabilities.Admission oxygen saturation on room air and patient age are strong predictors of deterioration and mortality among hospitalised adults with COVID-19, respectively. None of the prognostic models evaluated here offered incremental value for patient stratification to these univariable predictors.
Copyright ©ERS 2020.
Conflict of interest statement
Conflict of interest: M. Marks has nothing to disclose. Conflict of interest: T.H.A. Samuels has nothing to disclose. Conflict of interest: A. Luintel has nothing to disclose. Conflict of interest: T. Rampling has nothing to disclose. Conflict of interest: H. Chowdhury has nothing to disclose. Conflict of interest: M. Quartagno has nothing to disclose. Conflict of interest: A. Nair reports non-financial support from AIDENCE BV and grants from NIHR UCL Biomedical Research Centre, outside the submitted work. Conflict of interest: M. Lipman has nothing to disclose. Conflict of interest: I. Abubakar has nothing to disclose. Conflict of interest: M. van Smeden has nothing to disclose. Conflict of interest: W.K. Wong has nothing to disclose. Conflict of interest: B. Williams has nothing to disclose. Conflict of interest: M. Noursadeghi reports grants from Wellcome Trust and National Institute for Health Research Biomedical Research Centre at University College London NHS Foundation Trust, during the conduct of the study. Conflict of interest: R.K. Gupta has nothing to disclose.
Figures
Comment in
-
Performance of prediction models for COVID-19: the Caudine Forks of the external validation.Eur Respir J. 2020 Dec 24;56(6):2003728. doi: 10.1183/13993003.03728-2020. Print 2020 Dec. Eur Respir J. 2020. PMID: 33060155 Free PMC article.
References
-
- Imperial College COVID-19 Response Team Report 17 - Clinical characteristics and predictors of outcomes of hospitalised patients with COVID-19 in a London NHS Trust: a retrospective cohort study. www.imperial.ac.uk/mrc-global-infectious-disease-analysis/covid-19/repor.... Date last accessed: 14 May 2020. Date last updated: 29 April 2020.
-
- Li R, Rivers C, Tan Q, et al. The demand for inpatient and ICU beds for COVID-19 in the US: lessons from Chinese cities. medRxiv 2020; preprint [ 10.1101/2020.03.09.20033241]. - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous