

Recommendations for screening, monitoring, prevention, and prophylaxis of infections in adult and pediatric patients receiving CAR T-cell therapy: a position paper
- PMID: 32979154
- PMCID: PMC7518951
- DOI: 10.1007/s15010-020-01521-5
Recommendations for screening, monitoring, prevention, and prophylaxis of infections in adult and pediatric patients receiving CAR T-cell therapy: a position paper
Abstract
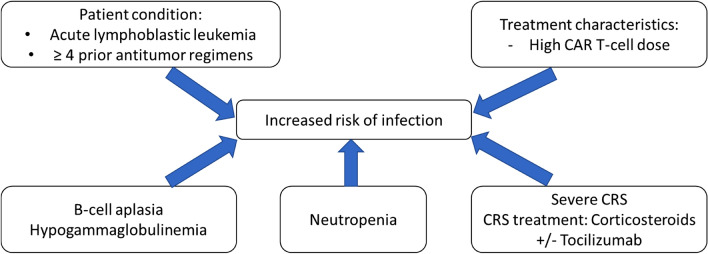
Chimeric antigen receptor (CAR) T-cell therapy is one of the most promising emerging treatments for B-cell malignancies. Recently, two CAR T-cell products (axicabtagene ciloleucel and tisagenlecleucel) have been approved for patients with aggressive B-cell lymphoma and acute lymphoblastic leukemia; many other CAR-T constructs are in research for both hematological and non-hematological diseases. Most of the patients receiving CAR-T therapy will develop fever at some point after infusion, mainly due to cytokine release syndrome (CRS). The onset of CRS is often indistinguishable from an infection, which makes management of these patients challenging. In addition to the lymphodepleting chemotherapy and CAR T cells, the treatment of complications with corticosteroids and/or tocilizumab increases the risk of infection in these patients. Data regarding incidence, risk factors and prevention of infections in patients receiving CAR-T cell therapy are scarce. To assist in patient care, a multidisciplinary team from hospitals designated by the Spanish Ministry of Health to perform CAR-T therapy prepared these recommendations. We reviewed the literature on the incidence, risk factors, and management of infections in adult and pediatric patients receiving CAR-T cell treatment. Recommendations cover different areas: monitoring and treatment of hypogammaglobulinemia, prevention, prophylaxis, and management of bacterial, viral, and fungal infections as well as vaccination prior and after CAR-T cell therapy.
Keywords: B-cell acute lymphoblastic leukemia; Bacterial infections; Chimeric antigen receptor; Diffuse large B-cell lymphoma; Fungal infections; Viral infections.
Conflict of interest statement
ILA declares having received travel support from Gilead, MSD and Novartis, and speaker honoraria from Pfizer, outside the submitted work. GI declares honoraria from Gilead, Novartis, Roche and Celgene. CDH declares having received travel grants from MSD, Gilead, Novartis Jazz Pharmaceuticals, Consultancy de Novartis and Amgen, and speaker fees from Novartis, Jazz Pharmaceuticals and Sobi. JLRO received travel grants from Novartis, Gilead and Celgene. VOM is a recipient of a research grant (FEHH), travel grants (Kite, Celgene, Novartis, Roche, Takeda & Janssen), consultant or advisory fees (Kite, Celgene, Novartis) and honoraria (Kite). PSP reports grants, personal fees and non-financial support from Gilead, Pfizer, MSD and Astellas Pharma, outside the submitted work. PB declares having received honoraria from Amgen, Celgene, Gilead, Incyte, Jazz Pharmaceuticals, MSD, Novartis, Pfizer and Roche, not related with the present article. IRC declares having received honoraria from, Celgene, Gilead, MSD, Astellas, Novartis, and Pfizer outside the submitted work. The rest of the authors declare that they have no conflict of interest.
Figures
References
-
- Bondanza A, Bonini C, Fehse B, Hudecek M. Cellular therapy with engineered T cells, efficacy and side effects. In: Carreras E, Dufour C, Mohty M, Kröger N, editors. The EBMT handbook. 7. Berlin: Springer; 2019. pp. 449–455. - PubMed
-
- Forman SJ, Kalos M, June CH. Adoptive T‐cell therapy for malignancy in the setting of hematopoietic cell transplantation. In: Antin JH, Appelbaum FR, Forman SJ, Negrin RS, editors. Thomas’ hematopoietic cell transplantion. 5th ed. Wiley-Blackwell; 2016. p. 826–35.
-
- Budde LE, Zaia JA. CD19 CAR-T therapy and sepsis: dancing with the devil. Blood. 2018;131:7–8. - PubMed
