

Significance of hematopoietic surface antigen CD34 in neuroblastoma prognosis and the genetic landscape of CD34-expressing neuroblastoma CSCs
- PMID: 32979173
- PMCID: PMC8529858
- DOI: 10.1007/s10565-020-09557-x
Significance of hematopoietic surface antigen CD34 in neuroblastoma prognosis and the genetic landscape of CD34-expressing neuroblastoma CSCs
Abstract
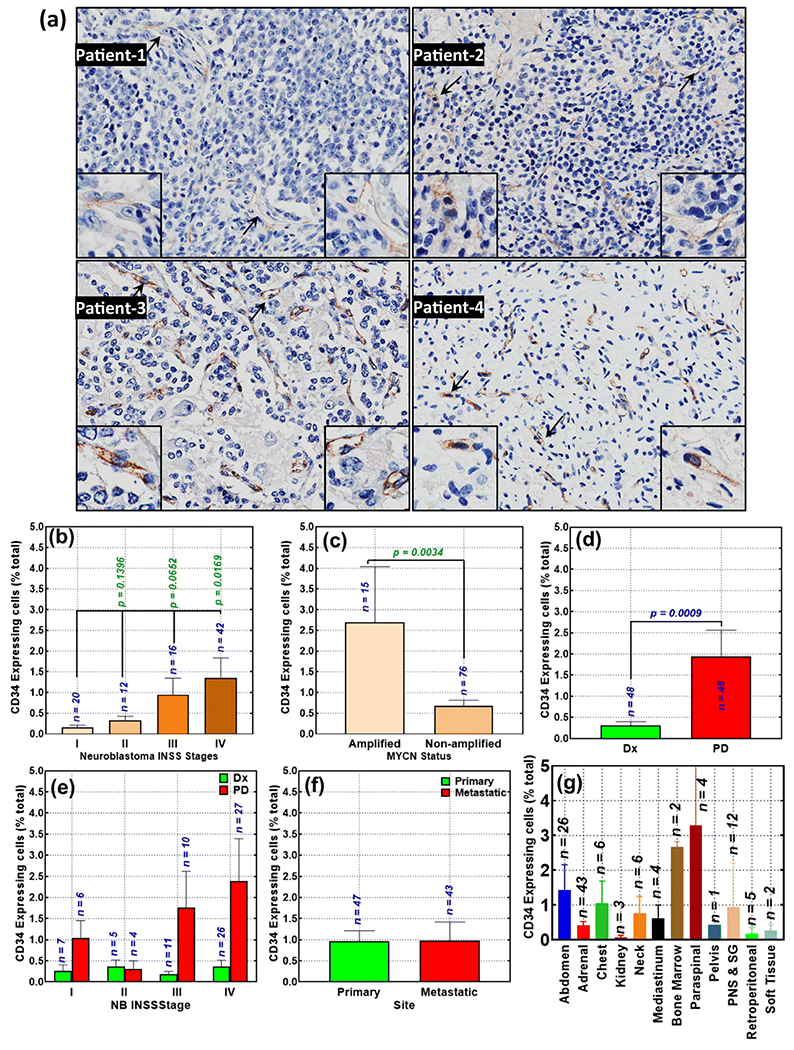
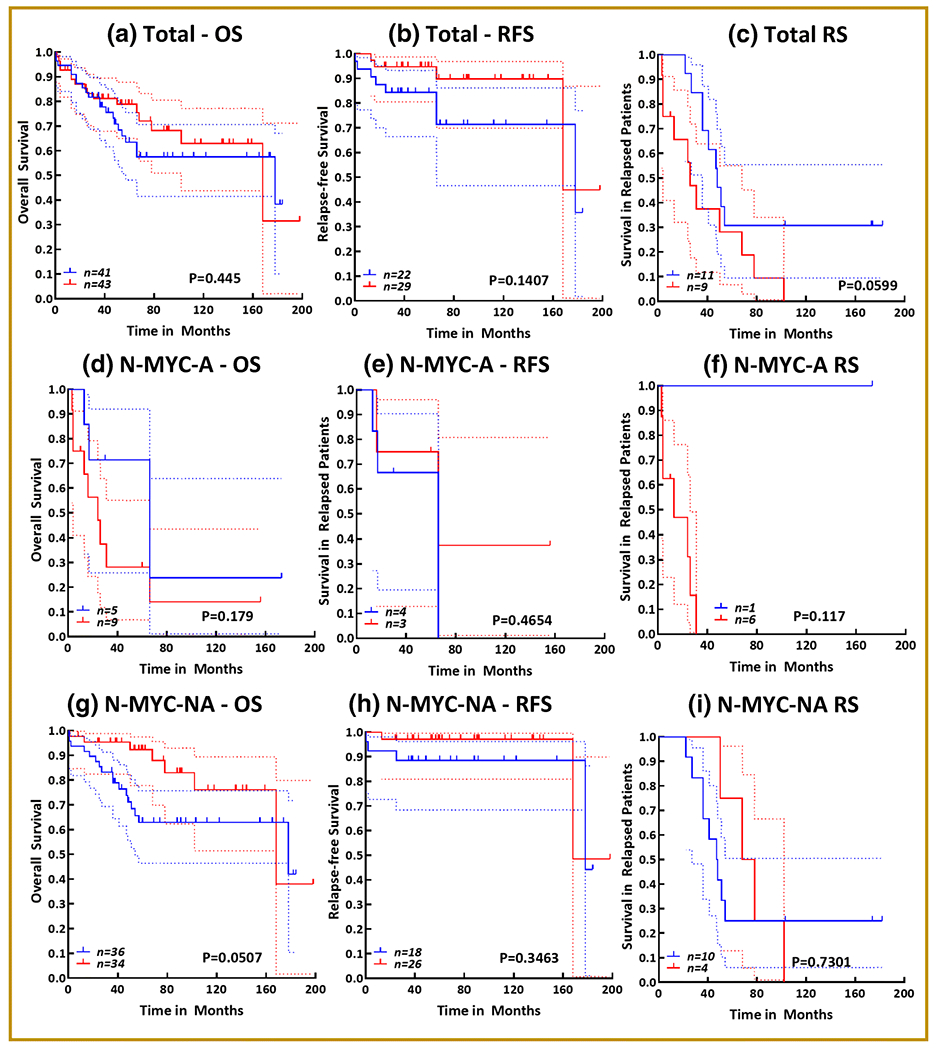
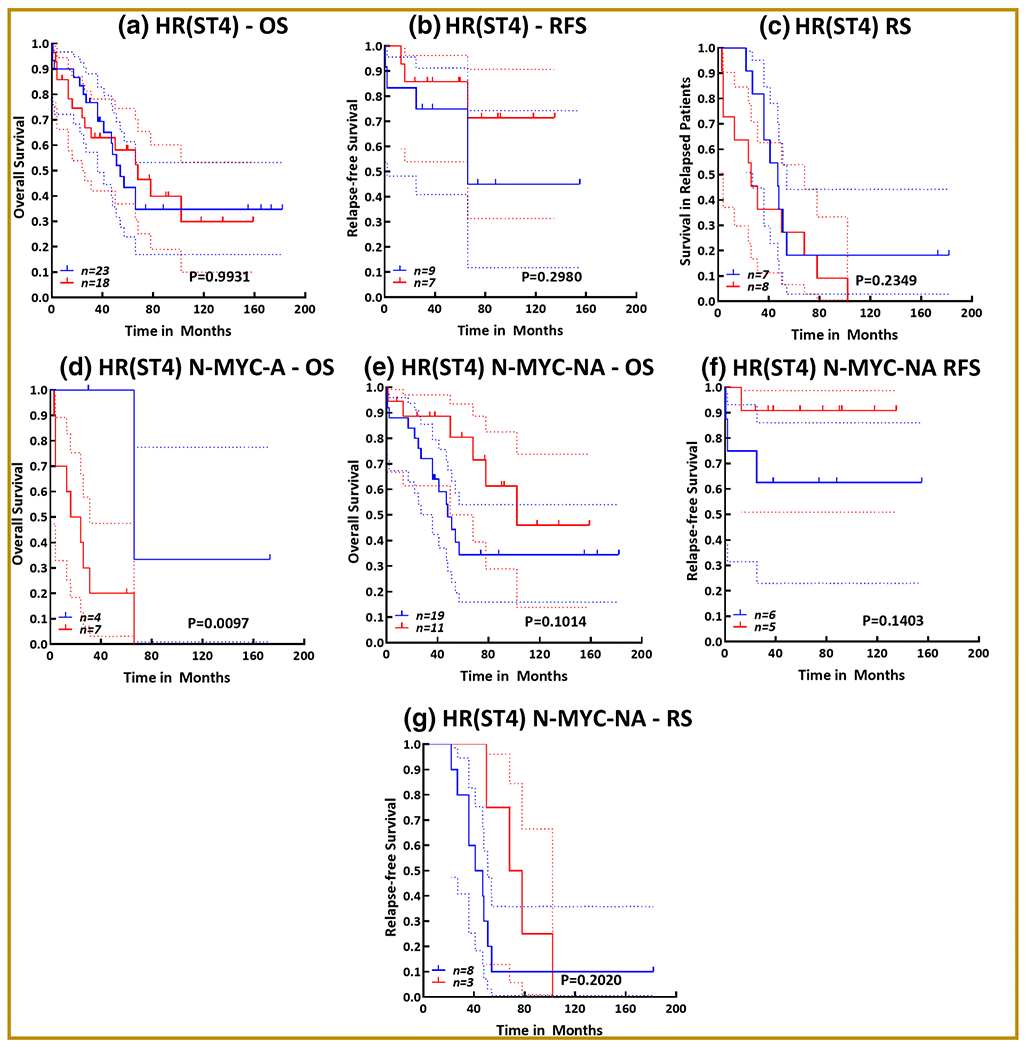
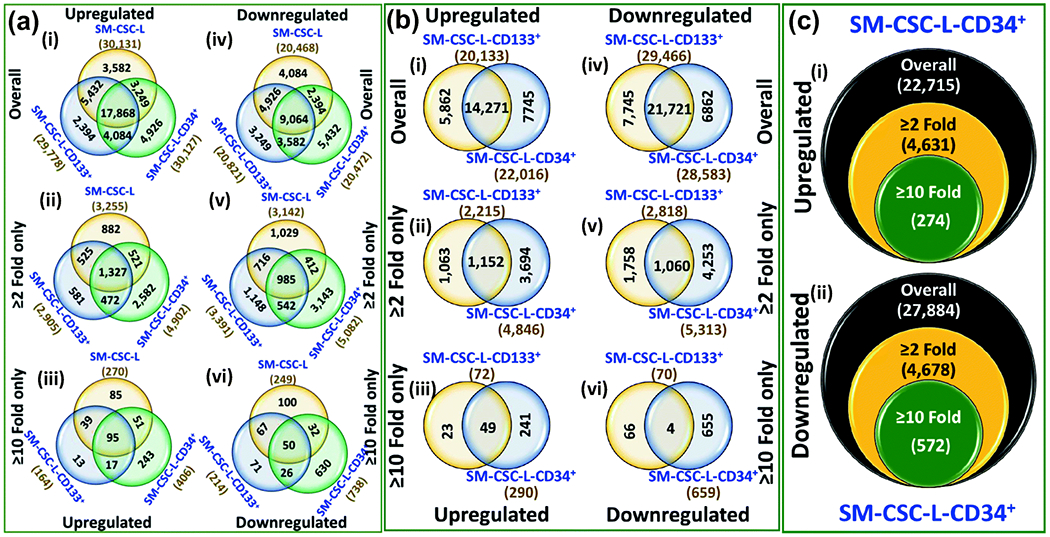
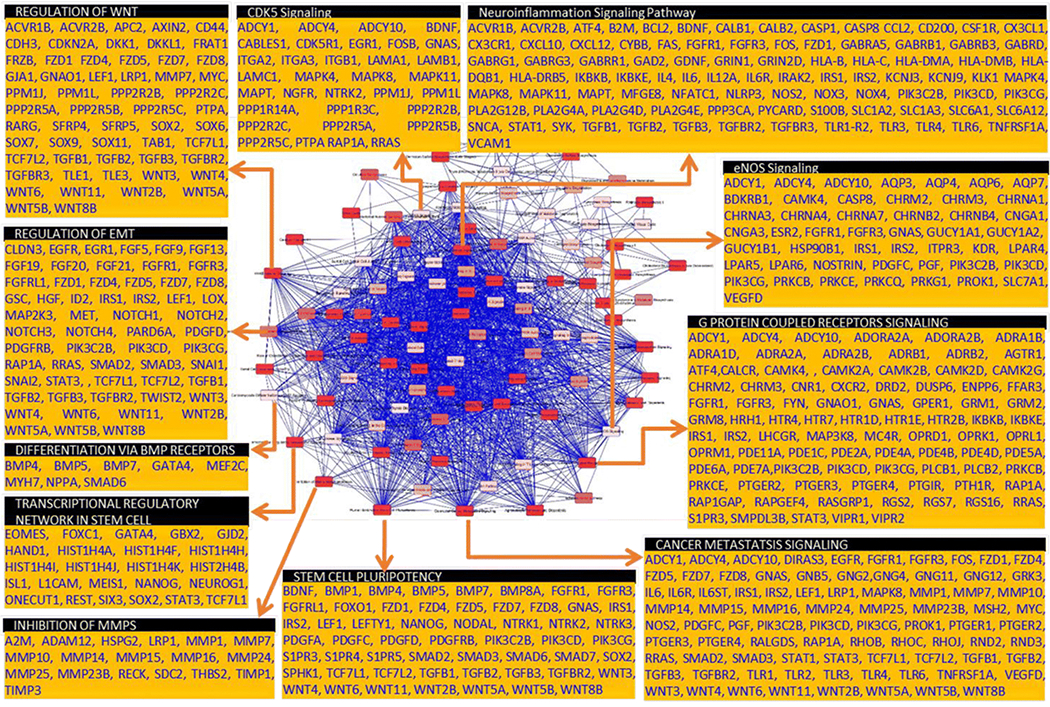
High-risk neuroblastoma (HR-NB) is branded with hematogenous metastasis, relapses, and dismal long-term survival. Intensification of consolidation therapy with tandem/triple autologous stem cell (SC) rescue (with bone marrow [BM]/peripheral blood [PB] CD34+ selection) after myeloablative chemotherapy has improved long-term survival. However, the benefit is limited by the indication of NB cells in CD34+ PBSCs, CD34 expression in NB cells, and the risk of reinfusing NB cancer stem cells (NB CSCs) that could lead to post-transplant relapse. We investigated the association of CD34 surface expression (92 patients) with NB evolution/clinical outcomes. CD34 gene-level status in NB was assessed through RNA-Seq data mining (18 cohorts, n, 3324). Genetic landscape of CD34-expressing NB CSCs (CD133+CD34+) was compared with CD34- CSCs (CD133+CD34-). RNA-seq data revealed equivocal association patterns of CD34 expression with patient survival. Our immunohistochemistry data revealed definite, but rare (mean, 0.73%; range 0.00-7.87%; median, 0.20%) CD34 positivity in NB. CD34+ significantly associated with MYCN amplification (p, 0.003), advanced disease stage (p, 0.016), and progressive disease (PD, p < 0.0009) after clinical therapy. A general high-is-worse tendency was observed in patients with relapsed disease. High CD34+ correlated with poor survival in patients with N-MYC-amplified HR-NB. Gene expression analysis of CD34+-NB CSCs identified significant up (4631) and downmodulation (4678) of genes compared with NB CSCs that lack CD34. IPA recognized the modulation of crucial signaling elements (EMT, stemness maintenance, differentiation, inflammation, clonal expansion, drug resistance, metastasis) that orchestrate NB disease evolution in CD34+ CSCs compared with CD34- CSCs. While the function of CD34 in NB evolution requires further in-depth investigation, careful consideration should be exercised for autologous stem cell rescue with CD34+ selection in NB patients. Graphical abstract.
Keywords: CD34; Cancer stem cells; Disease evolution; Neuroblastoma; Stem cell rescue; Tumor progression.
Conflict of interest statement
Figures
References
-
- Ahmed AA, Zhang L, Reddivalla N, Hetherington M (2017). Neuroblastoma in children: Update on clinicopathologic and genetic prognostic factors. Pediatr Hematol Oncol 34:165–185 - PubMed
-
- Ambros PF, Ambros IM, Brodeur GM, Haber M, Khan J, Nakagawara A, Schleiermacher G, Speleman F, Spitz R, London WB, Cohn SL, Pearson AD, Maris JM (2009). International consensus for neuroblastoma molecular diagnostics: report from the International Neuroblastoma Risk Group (INRG) Biology Committee. Br J Cancer 100:1471–82 - PMC - PubMed
-
- American-Cancer-Society. (2013). Cancer Facts & Figures Atlanta: American Cancer Society 1–64
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
