

Trends and Outcomes in Minimally Invasive Surgery for Locally Advanced Non-Small-Cell Lung Cancer With N2 Disease
- PMID: 32979480
- PMCID: PMC10715223
- DOI: 10.1053/j.semtcvs.2020.09.008
Trends and Outcomes in Minimally Invasive Surgery for Locally Advanced Non-Small-Cell Lung Cancer With N2 Disease
Abstract
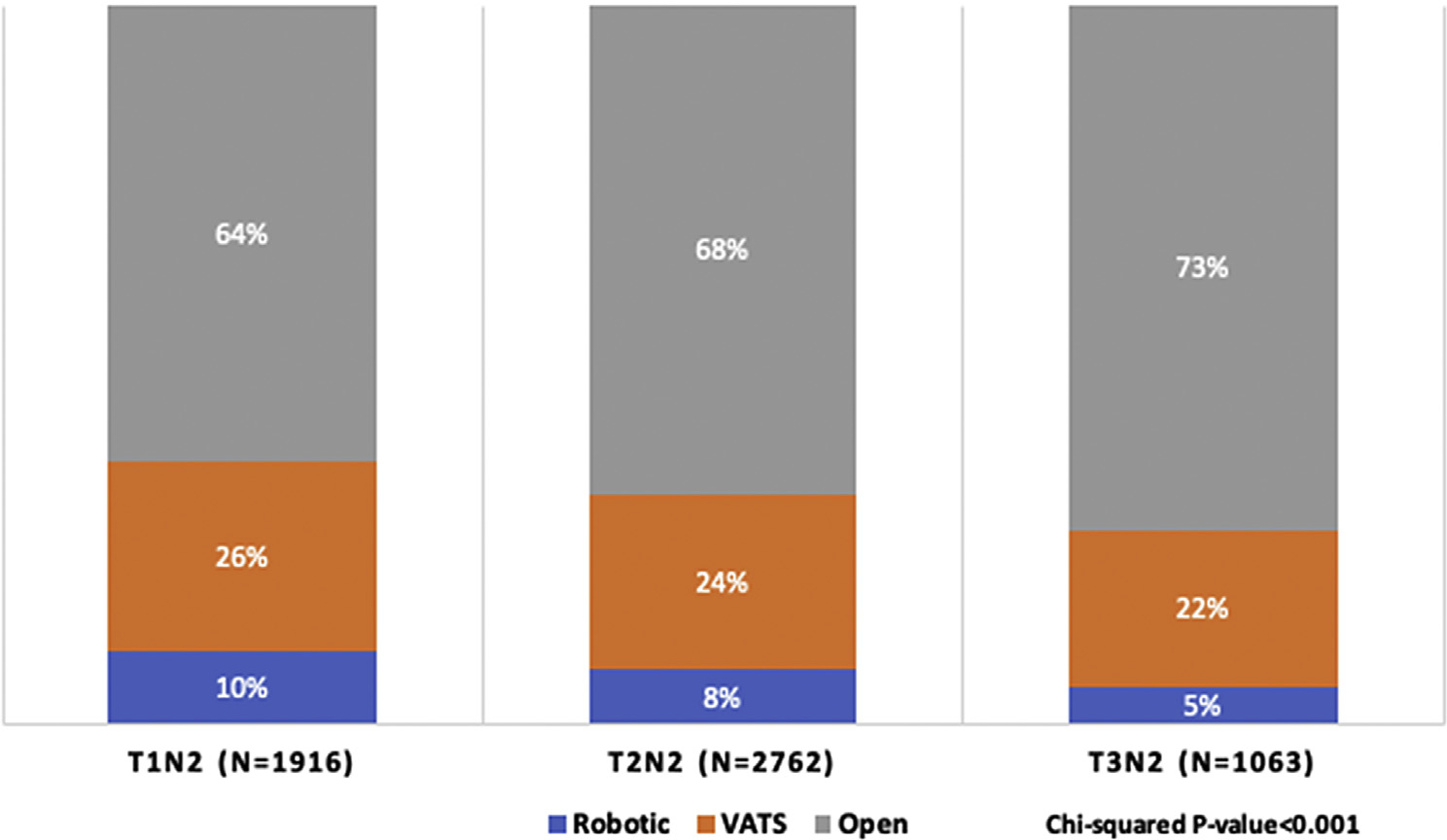
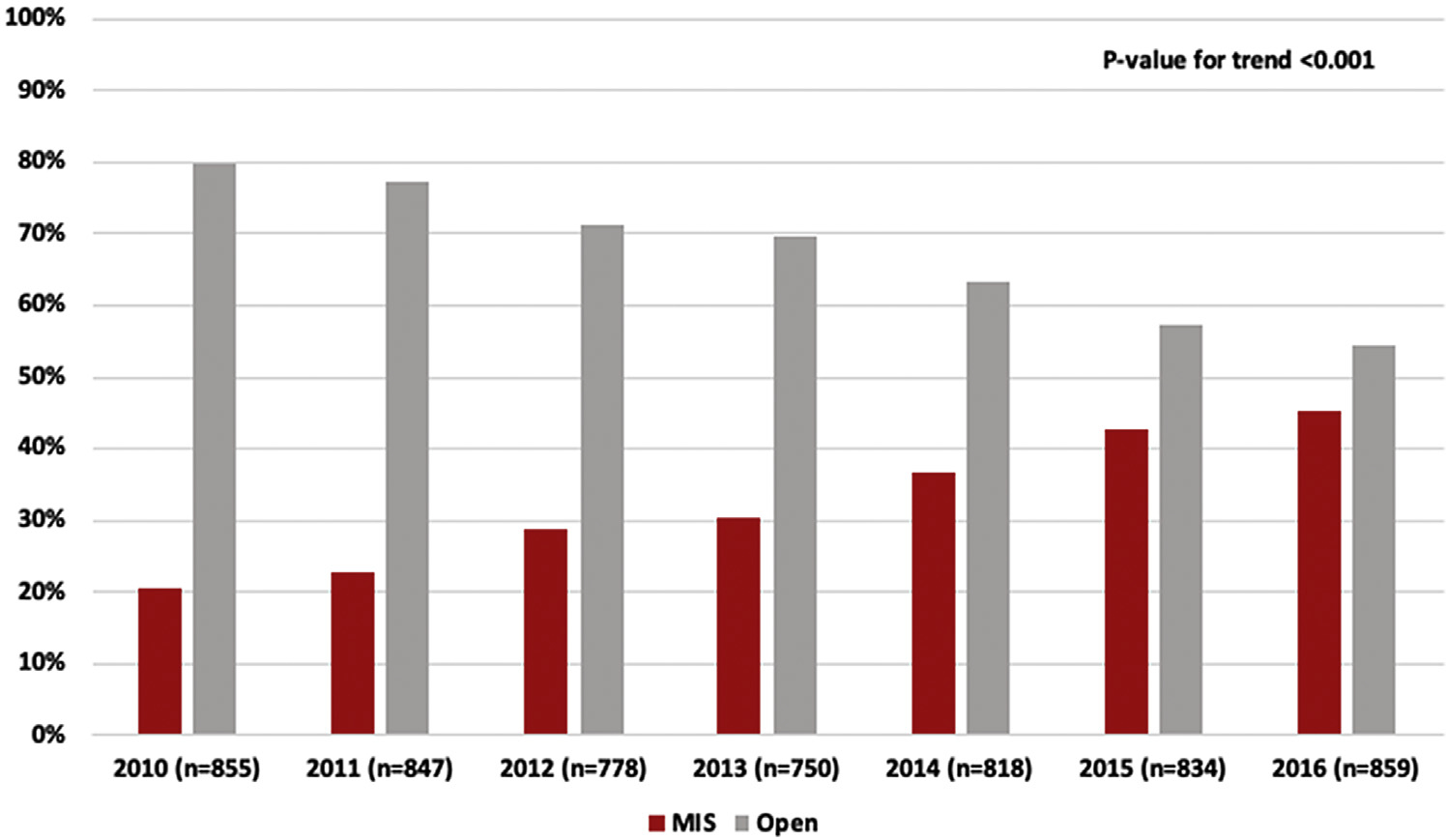
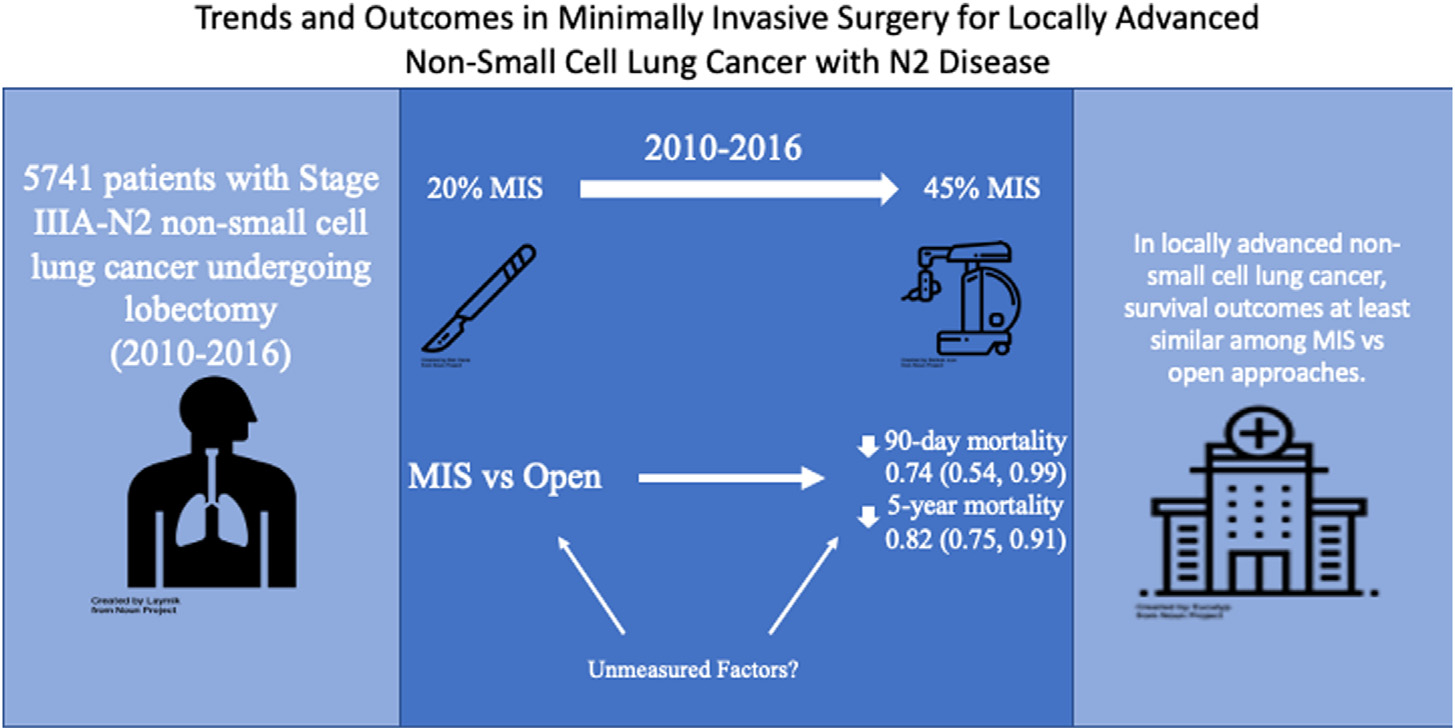
Few studies examine outcomes by surgical approach in non-small-cell lung cancer (NSCLC) with N2 disease. We examined time trends in surgical approach and outcomes among patients undergoing minimally invasive (MIS, robotic and video-assisted thoracoscopic surgery [VATS]) vs open lobectomy in this patient population. We performed a retrospective analysis of patients from the National Cancer Database diagnosed with clinical Stage IIIA-N2 NSCLC from 2010 to 2016. We examined the yearly proportion of MIS vs open resections. Multivariable regression was used to assess the association of surgical approach with length of stay, unplanned readmissions, 30-day and 90-day mortality. Multivariable Cox proportional hazards modeling was used to assess the association of surgical approach with 5-year overall mortality. We identified 5741 patients who underwent lobectomy for Stage IIIA-N2 NSCLC (459 robotic, 1403 VATS, 3879 open). From 2010 to 2016, the proportion of minimally invasive procedures increased from 20% to 45%. MIS patients, on average, stayed 1 day less in the hospital (95% confidence interval [CI] 0.7, 1.5) and had lower odds of 90-day (odds ratio [OR] 0.74; 95% CI 0.54, 0.99) and 5-year mortality (OR 0.82; 95% CI 0.75, 0.91), compared to open resections. There was no difference in odds of readmission by surgical approach (OR 0.97; 95% CI 0.71, 1.33). Among MIS procedures, robotic resections had lower odds of 90-day mortality (OR 0.42; 95% CI 0.18, 0.97) than VATS. Among patients undergoing lobectomy for locally advanced N2 NSCLC robotic and VATS techniques appear safe and effective compared to open surgery and may offer short- and long-term advantages.
Keywords: Locally advanced non–small-cell lung cancer; Minimally invasive surgery.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to report.
Figures
Comment in
-
Commentary: I Am Happy to Inform You That Thoracotomy Is No Longer Required for Stage IIIA-N2 NSCLC.Semin Thorac Cardiovasc Surg. 2021 Summer;33(2):558. doi: 10.1053/j.semtcvs.2020.10.036. Epub 2020 Nov 9. Semin Thorac Cardiovasc Surg. 2021. PMID: 33181292 No abstract available.
-
Commentary: Minimally Invasive Surgery in N2 Stage IIIA Lung Cancer: Time for Caution Not Time to Throw Caution to the Wind.Semin Thorac Cardiovasc Surg. 2021 Summer;33(2):556-557. doi: 10.1053/j.semtcvs.2020.10.046. Epub 2020 Nov 13. Semin Thorac Cardiovasc Surg. 2021. PMID: 33197568 No abstract available.
References
-
- National Comprehensive Cancer Network. Non-small cell lung cancer (v2.2019). Available at: https://www.nccn.org/professionals/physician_gls/PDF/nscl.pdf. 2019. Accessed January 31, 2019
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
