

Pharmacologic treatment of orthostatic hypotension
- PMID: 32979782
- PMCID: PMC7704612
- DOI: 10.1016/j.autneu.2020.102721
Pharmacologic treatment of orthostatic hypotension
Abstract
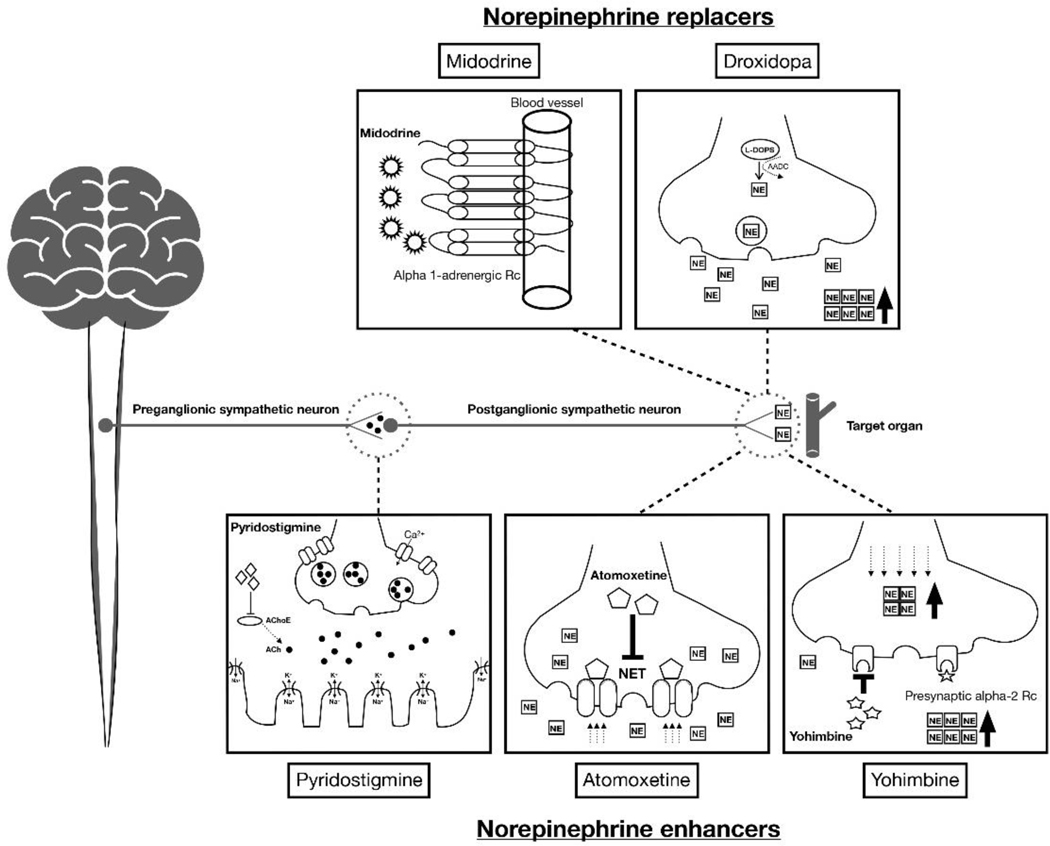
Neurogenic orthostatic hypotension (OH) is a disabling disorder caused by impairment of the normal autonomic compensatory mechanisms that maintain upright blood pressure. Nonpharmacologic treatment is always the first step in the management of this condition, but a considerable number of patients will require pharmacologic therapies. Denervation hypersensitivity and impairment of baroreflex buffering makes these patients sensitive to small doses of pressor agents. Understanding the underlying pathophysiology can help in selecting between treatment options. In general, patients with low "sympathetic reserve", i.e., those with peripheral noradrenergic degeneration (pure autonomic failure, Parkinson's disease) and low plasma norepinephrine, tend to respond better to "norepinephrine replacers" (midodrine and droxidopa). On the other hand, patients with relatively preserved "sympathetic reserve", i.e., those with impaired central autonomic pathways but spared peripheral noradrenergic fibers (multiple system atrophy) and normal or slightly reduced plasma norepinephrine, tend to respond better to "norepinephrine enhancers" (pyridostigmine, atomoxetine, and yohimbine). There is, however, a spectrum of responses within these extremes, and treatment should be individualized. Other nonspecific treatments include fludrocortisone and octreotide. The presence of associated clinical conditions, such as supine hypertension, heart failure, postprandial hypotension, PD, MSA, and diabetes need to be considered in the pharmacologic management of these patients.
Keywords: Orthostatic hypotension; Pharmacologic treatment.
Copyright © 2020 Elsevier B.V. All rights reserved.
Figures
Similar articles
-
Efficacy of atomoxetine versus midodrine for the treatment of orthostatic hypotension in autonomic failure.Hypertension. 2014 Dec;64(6):1235-40. doi: 10.1161/HYPERTENSIONAHA.114.04225. Epub 2014 Sep 2. Hypertension. 2014. PMID: 25185131 Free PMC article. Clinical Trial.
-
[Orthostatic hypotension and supine hypertension in primary autonomic failure. Pathophysiology, diagnosis and treatment].Kardiol Pol. 2010 Sep;68(9):1057-63. Kardiol Pol. 2010. PMID: 20859904 Review. Polish.
-
Association between supine hypertension and orthostatic hypotension in autonomic failure.Hypertension. 2003 Aug;42(2):136-42. doi: 10.1161/01.HYP.0000081216.11623.C3. Epub 2003 Jun 30. Hypertension. 2003. PMID: 12835329
-
Long-term safety of droxidopa in patients with symptomatic neurogenic orthostatic hypotension.J Am Soc Hypertens. 2016 Oct;10(10):755-762. doi: 10.1016/j.jash.2016.07.010. Epub 2016 Aug 4. J Am Soc Hypertens. 2016. PMID: 27614923 Clinical Trial.
-
Diagnosing and treating neurogenic orthostatic hypotension in primary care.Postgrad Med. 2015;127(7):702-15. doi: 10.1080/00325481.2015.1050340. Epub 2015 May 27. Postgrad Med. 2015. PMID: 26012731 Review.
Cited by
-
Updates on the Diagnosis and Treatment of Peripheral Autonomic Neuropathies.Curr Neurol Neurosci Rep. 2022 Dec;22(12):823-837. doi: 10.1007/s11910-022-01240-4. Epub 2022 Nov 15. Curr Neurol Neurosci Rep. 2022. PMID: 36376534 Free PMC article. Review.
-
Orthostatic Hypotension in Parkinson Disease: What Is New?Neurol Clin Pract. 2022 Oct;12(5):e112-e115. doi: 10.1212/CPJ.0000000000200068. Neurol Clin Pract. 2022. PMID: 36380891 Free PMC article.
-
Cardiovascular Autonomic Dysfunction Before and After Chemotherapy in Cancer Patients.J Clin Neurol. 2024 Nov;20(6):551-562. doi: 10.3988/jcn.2024.0221. J Clin Neurol. 2024. PMID: 39505307 Free PMC article. Review.
-
Use of Valsalva Maneuver to Detect Late-Onset Delayed Orthostatic Hypotension.Hypertension. 2023 Apr;80(4):792-801. doi: 10.1161/HYPERTENSIONAHA.122.20098. Epub 2023 Jan 25. Hypertension. 2023. PMID: 36695176 Free PMC article. Clinical Trial.
-
Fludrocortisone Induces Aortic Pathologies in Mice.Biomolecules. 2022 Jun 13;12(6):825. doi: 10.3390/biom12060825. Biomolecules. 2022. PMID: 35740952 Free PMC article.
References
-
- Agarwal S, Gowda KV, Mandal U, Ghosh D, Bose A, Sarkar AK, Pal TK, Chattaraj TK 2007. Analysis of pyridostigmine bromide in human plasma and its application in bioequivalence studies. Journal of liquid chromatography & related technologies 30, 2605–2615.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
