

17-Hydroxyprogesterone caproate improves hypertension and renal endothelin-1 in response to sFlt-1 induced hypertension in pregnant rats
- PMID: 32980622
- PMCID: PMC10278054
- DOI: 10.1016/j.preghy.2020.09.002
17-Hydroxyprogesterone caproate improves hypertension and renal endothelin-1 in response to sFlt-1 induced hypertension in pregnant rats
Abstract
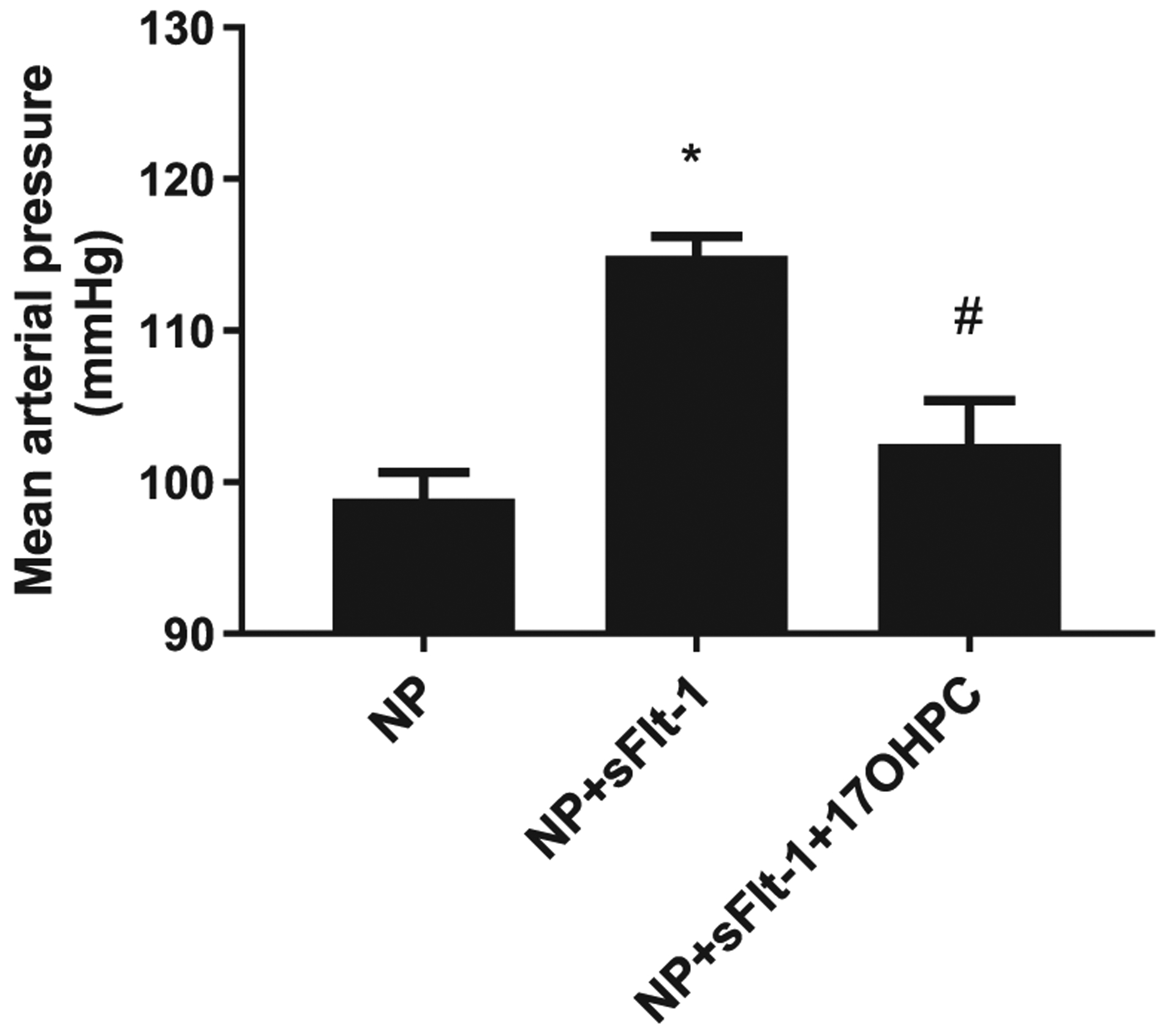
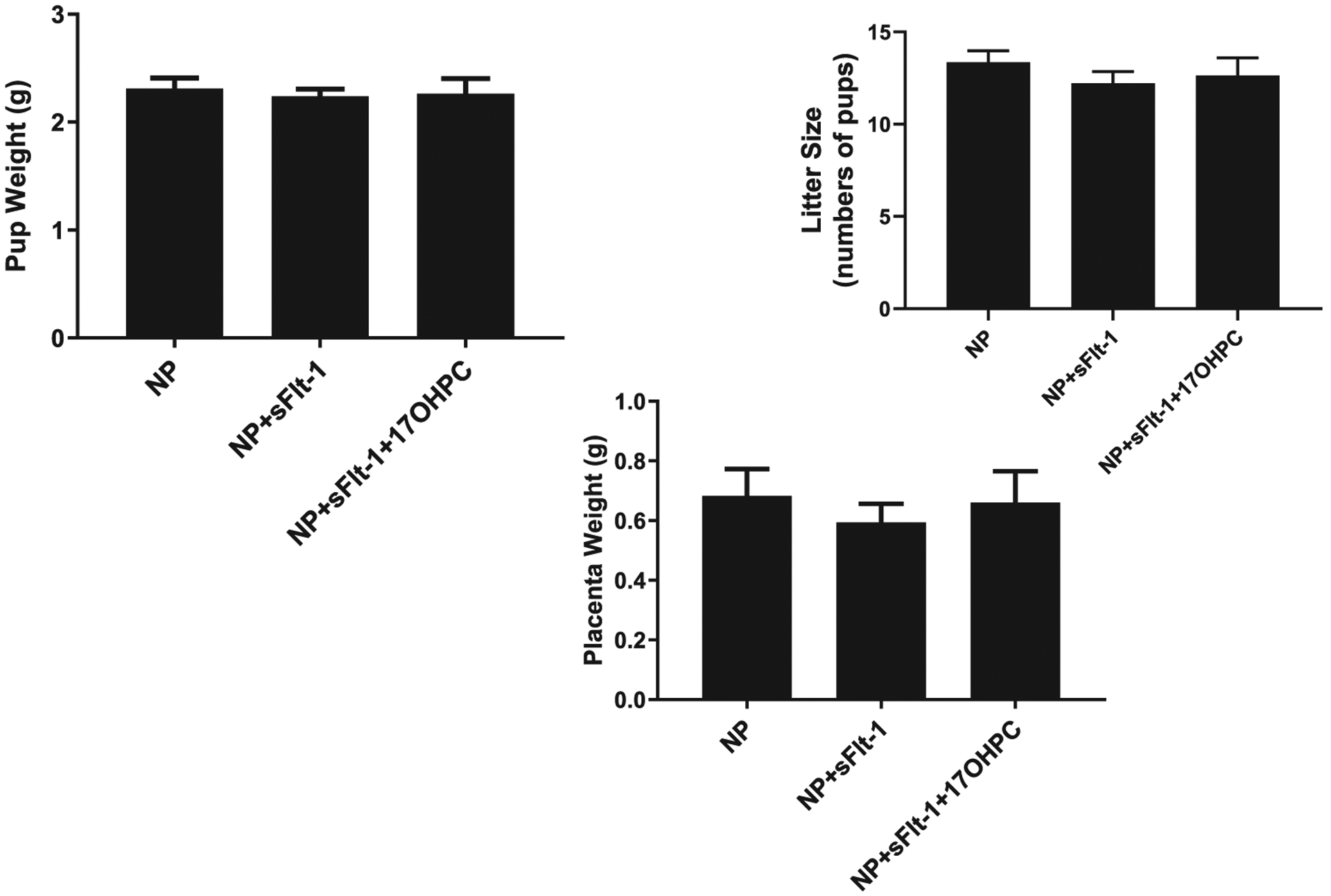
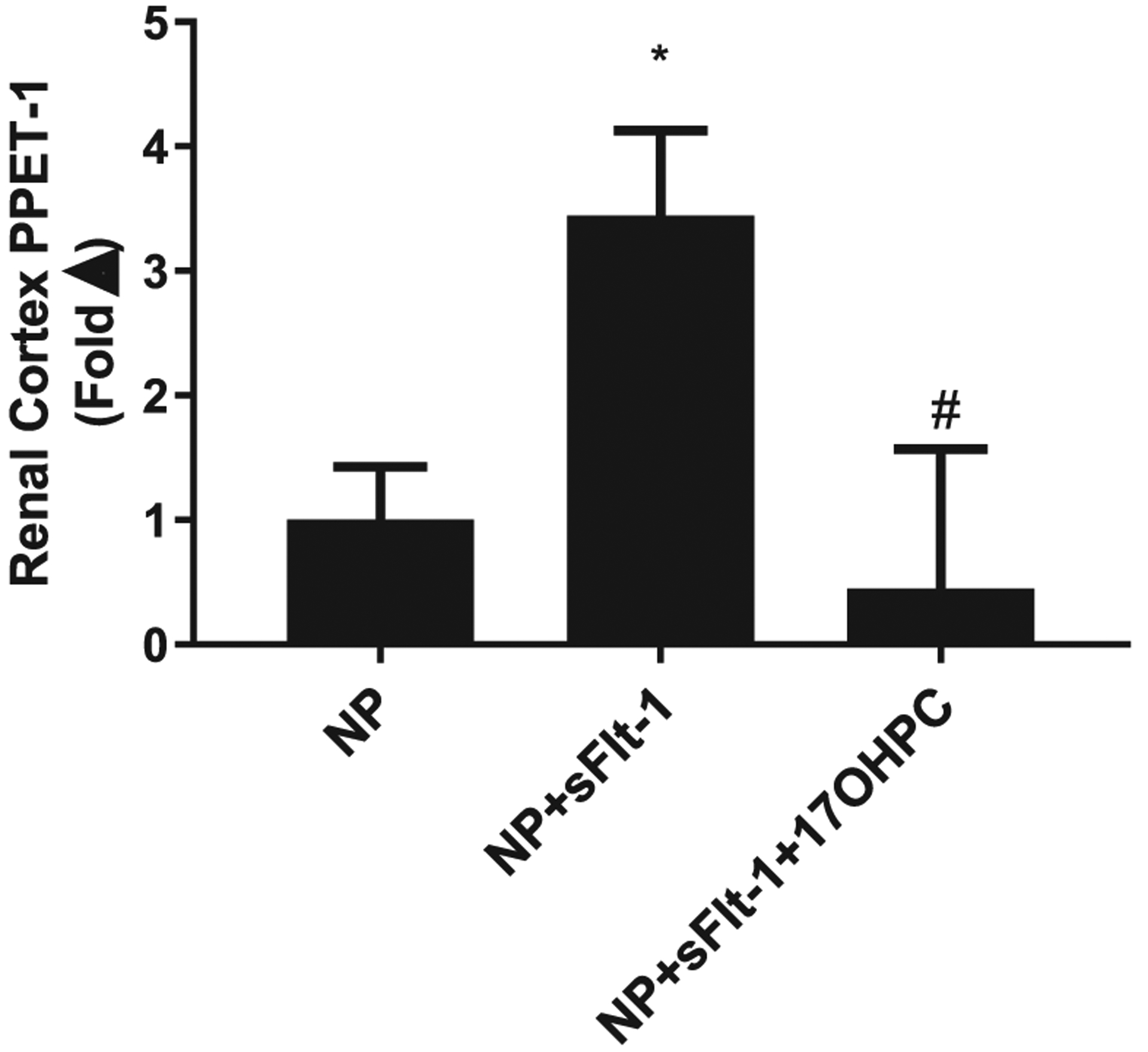
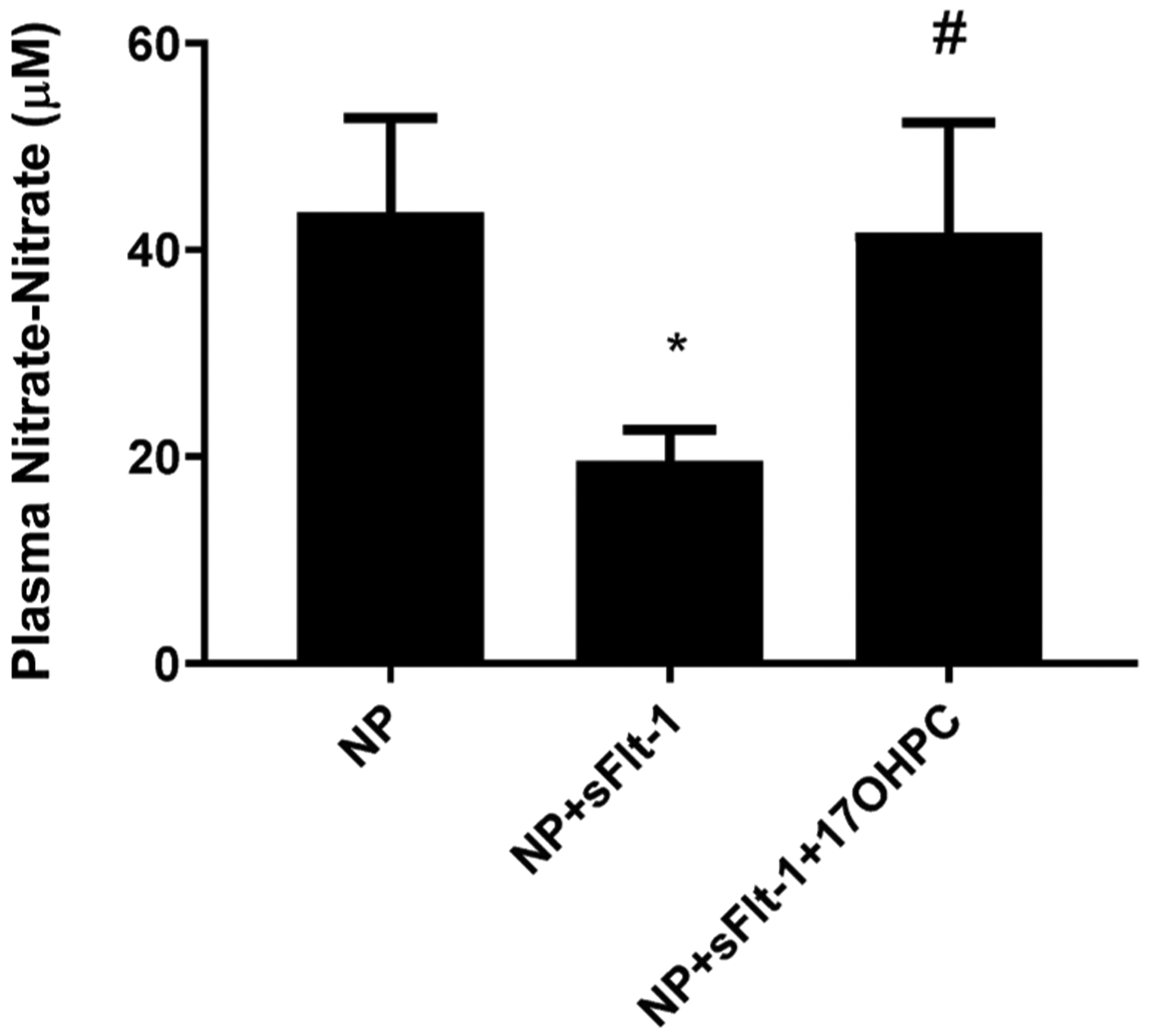
Preeclampsia (PE) is characterized by new onset hypertension in association with elevated soluble fms-like tyrosine kinase-1 (sFlt-1) and preproendothelin-1 (PPET-1) levels. Currently there is no effective treatment for PE except for early delivery of the fetal placental unit, making PE a leading cause for premature births worldwide. Administration of 17-hydroxyprogesterone caproate (17-OHPC) is used for prevention of recurrent preterm birth. This study was designed to test the hypothesis that 17-OHPC improves hypertension and ET-1 in response to elevated sFlt-1 in pregnant rats. sFlt-1 was infused into normal pregnant (NP) Sprague-Dawley rats (3.7 μg·kg-1·day-1 for 6 days, gestation days 13-19) in the presence or absence of 17-OHPC (3.32 mg/kg) administered via intraperitoneal injection on gestational days 15 and 18. Mean arterial blood pressure (MAP), pup and placenta weights, renal cortex PPET-1 mRNA levels and nitrate-nitrite levels were measured on GD 19. Infusion of sFlt-1 into NP rats elevated mean arterial pressure (MAP) compared with control NP rats: 115 ± 1 (n = 13) vs. 99 ± 2 mmHg (n = 12, p < 0.05). 17-OHPC attenuated this hypertension reducing MAP to 102 ± 3 mmHg in sFlt-1 treated pregnant rats (n = 8). Neither pup nor placental weight was affected by sFlt-1 or 17-OHPC. Importantly, renal cortex PPET-1 mRNA levels were elevated 3 fold in NP + sFlt-1 rats compare to NP rats, which decreased with 17-OHPC administration. Plasma nitrate-nitrite levels were 44 ± 9 µM in NP rats (n = 9), 20 ± 3 µM in NP + sFlt-1 (n = 7), which increased to 42 ± 11 µM NP + sFlt-1 + 17OHPC (n = 6). Administration of 17-OHPC improves clinical characteristics of preeclampsia in response to elevated sFlt-1 during pregnancy.
Keywords: 17-OHPC; Preeclampsia; Preproendothelin-1; sFlt-1.
Copyright © 2020 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Creasy RK, Resnik R, Greene MF, Iams JD, Lockwood CJ, Creasy and resnik’s maternal-fetal medicine: principles and practice.1 online resource.
-
- Duley L, Maternal mortality associated with hypertensive disorders of pregnancy in africa, asia, latin america and the caribbean, Br. J. Obstet. Gynaecol 99 (1992) 547–553. - PubMed
-
- Noris M, Perico N, Remuzzi G, Mechanisms of disease: pre-eclampsia, Nat. Clin. Practice Nephrol 1 (2005) 98–114, quiz 120. - PubMed
-
- American College of O, Gynecologists, Task Force on Hypertension in P. Hypertension in pregnancy. Report of the American college of obstetricians and gynecologists’ task force on hypertension in pregnancy. Obstet. Gynecol 122 (2013) 1122–1131. - PubMed
-
- Schlembach D, Pre-eclampsia–still a disease of theories, Fukushima J. Med. Sci 49 (2003) 69–115. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
