

Deterministic linear Boltzmann transport equation solver for patient-specific CT dose estimation: Comparison against a Monte Carlo benchmark for realistic scanner configurations and patient models
- PMID: 32981038
- PMCID: PMC7837758
- DOI: 10.1002/mp.14494
Deterministic linear Boltzmann transport equation solver for patient-specific CT dose estimation: Comparison against a Monte Carlo benchmark for realistic scanner configurations and patient models
Abstract
Purpose: Epidemiological evidence suggests an increased risk of cancer related to computed tomography (CT) scans, with children exposed to greater risk. The purpose of this work is to test the reliability of a linear Boltzmann transport equation (LBTE) solver for rapid and patient-specific CT dose estimation. This includes building a flexible LBTE framework for modeling modern clinical CT scanners and to validate the resulting dose maps across a range of realistic scanner configurations and patient models.
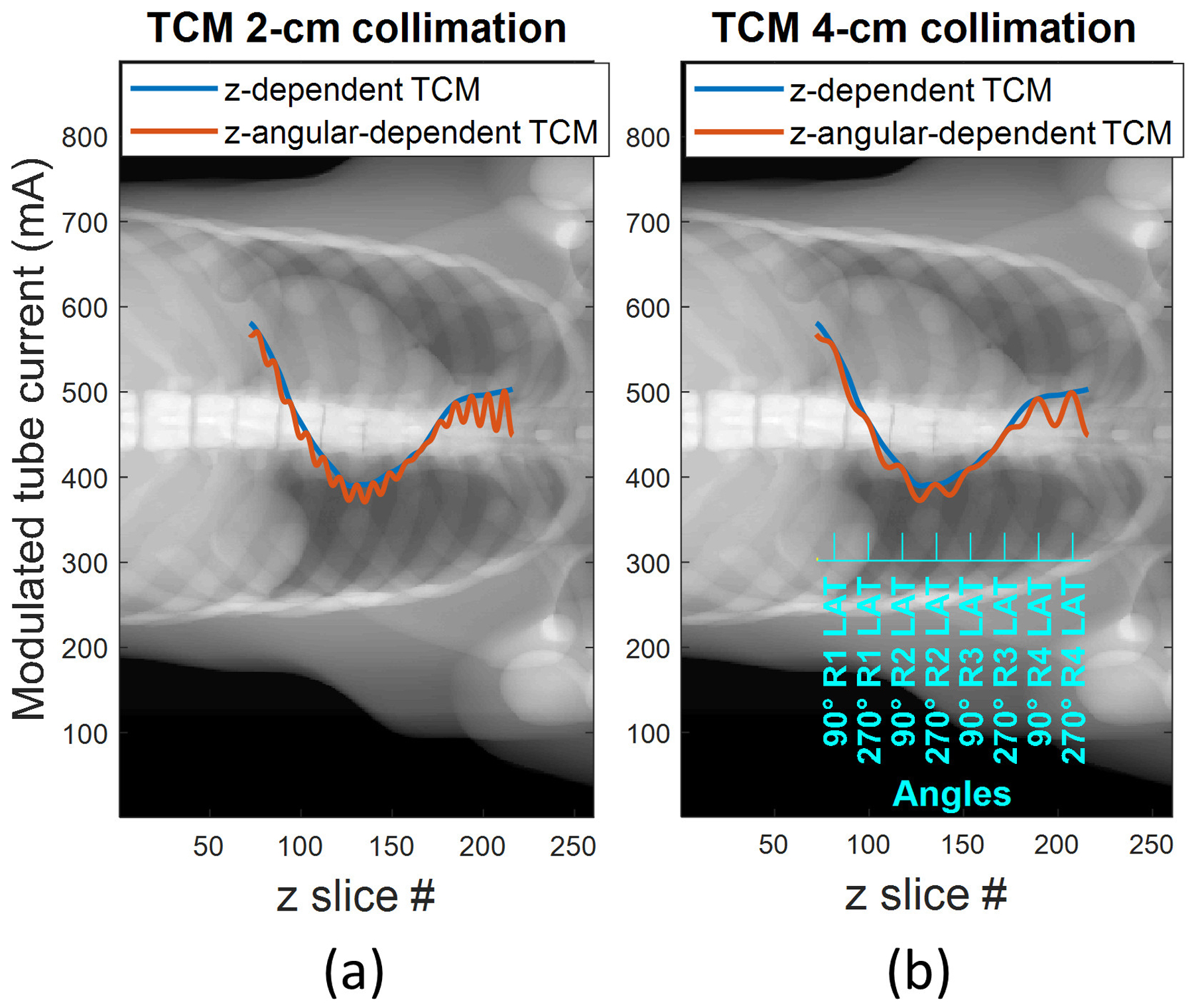
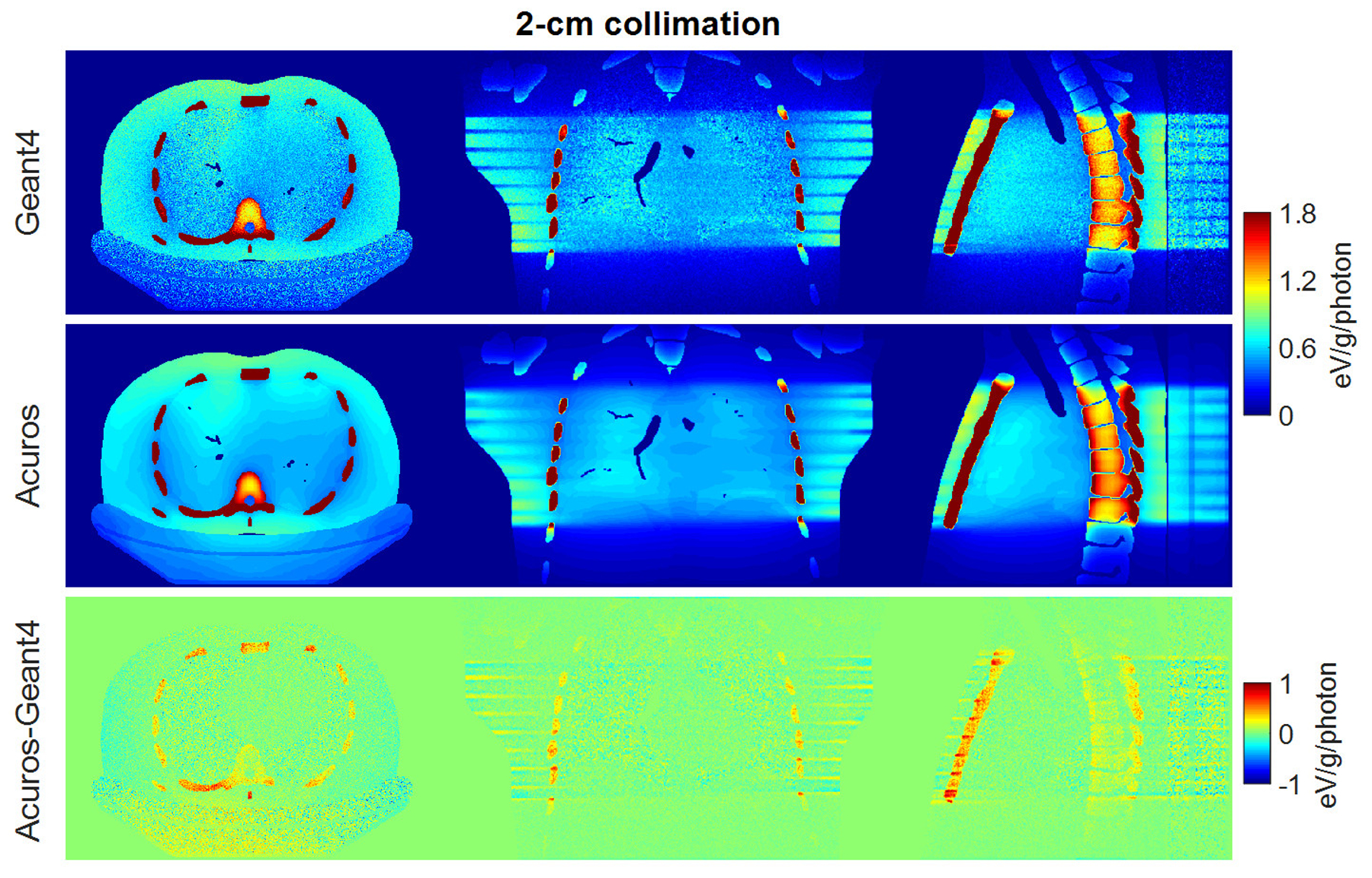
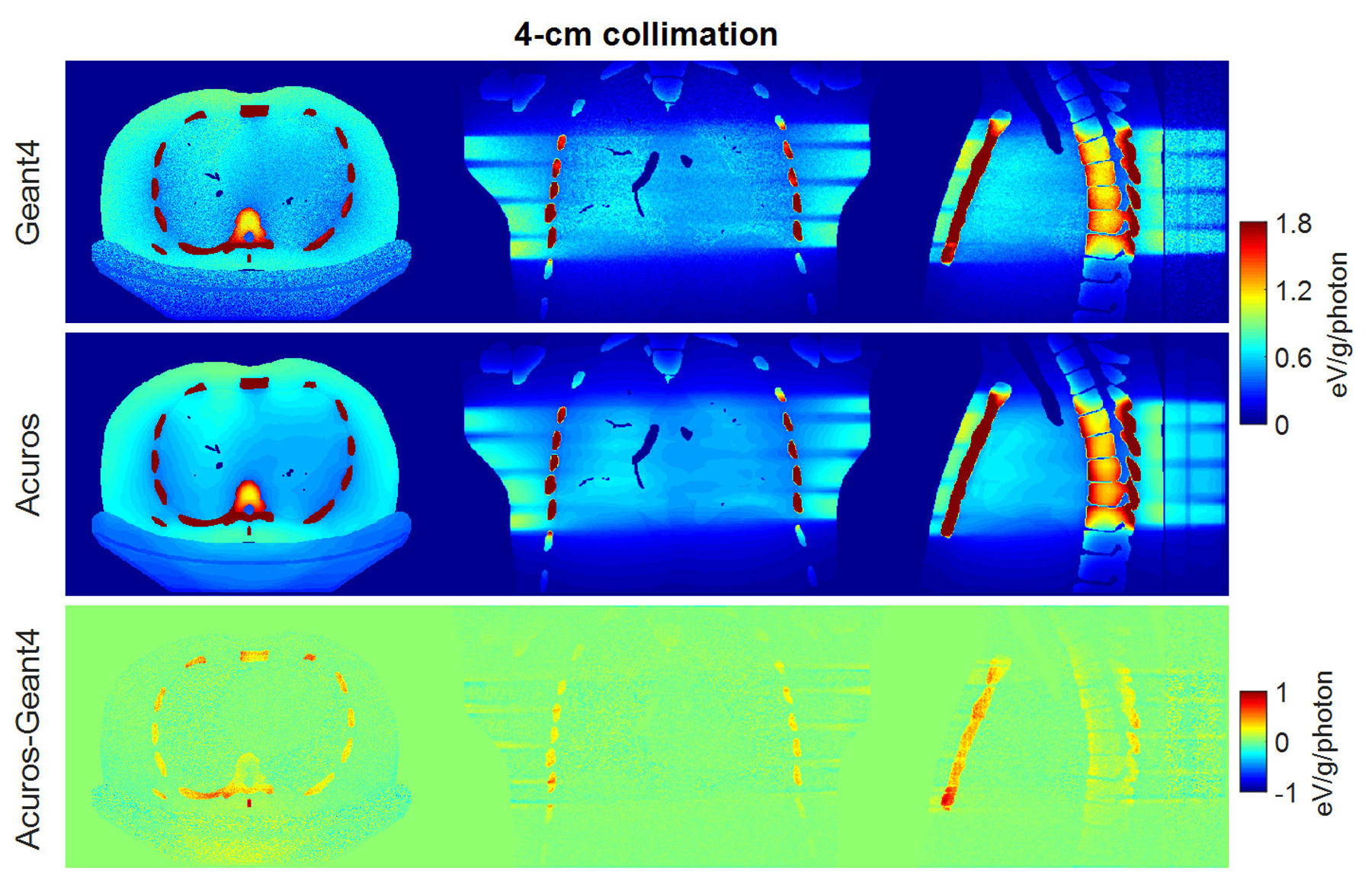
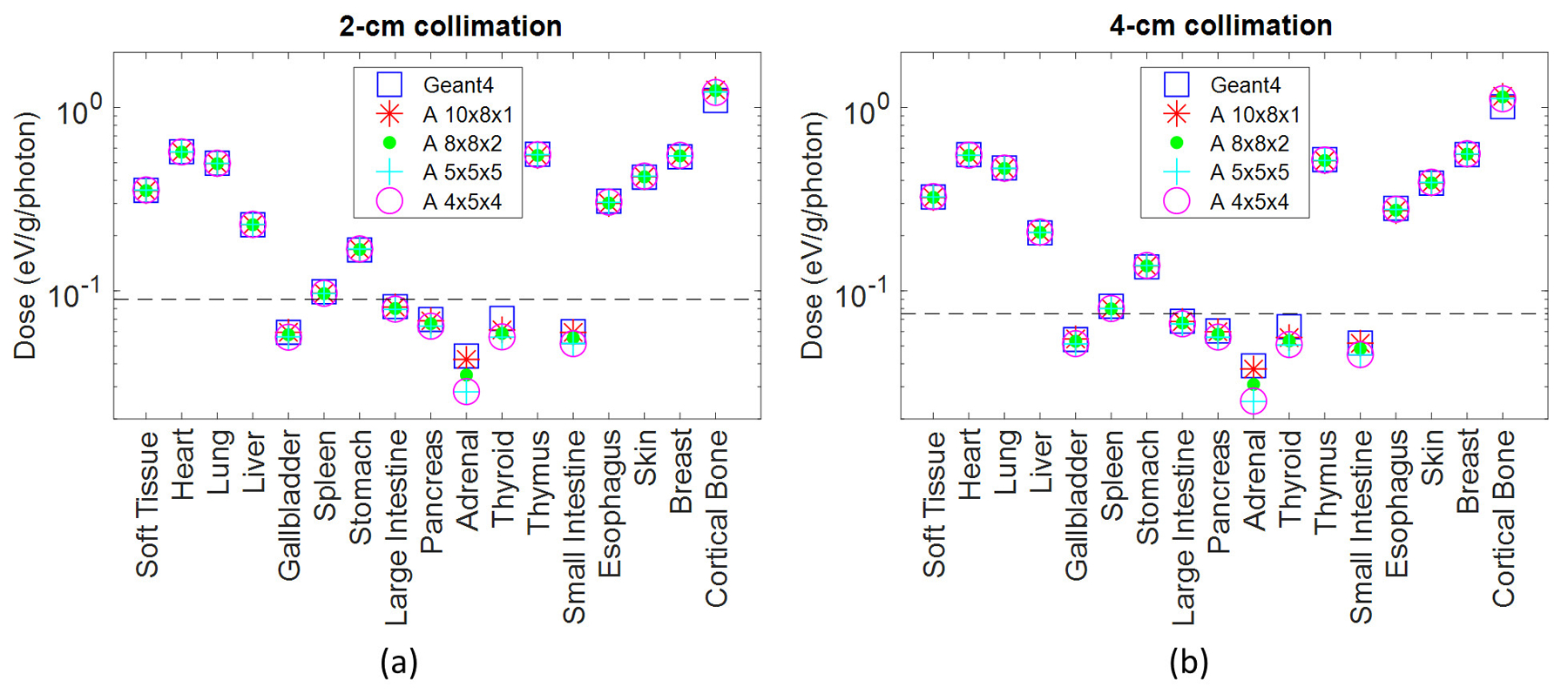
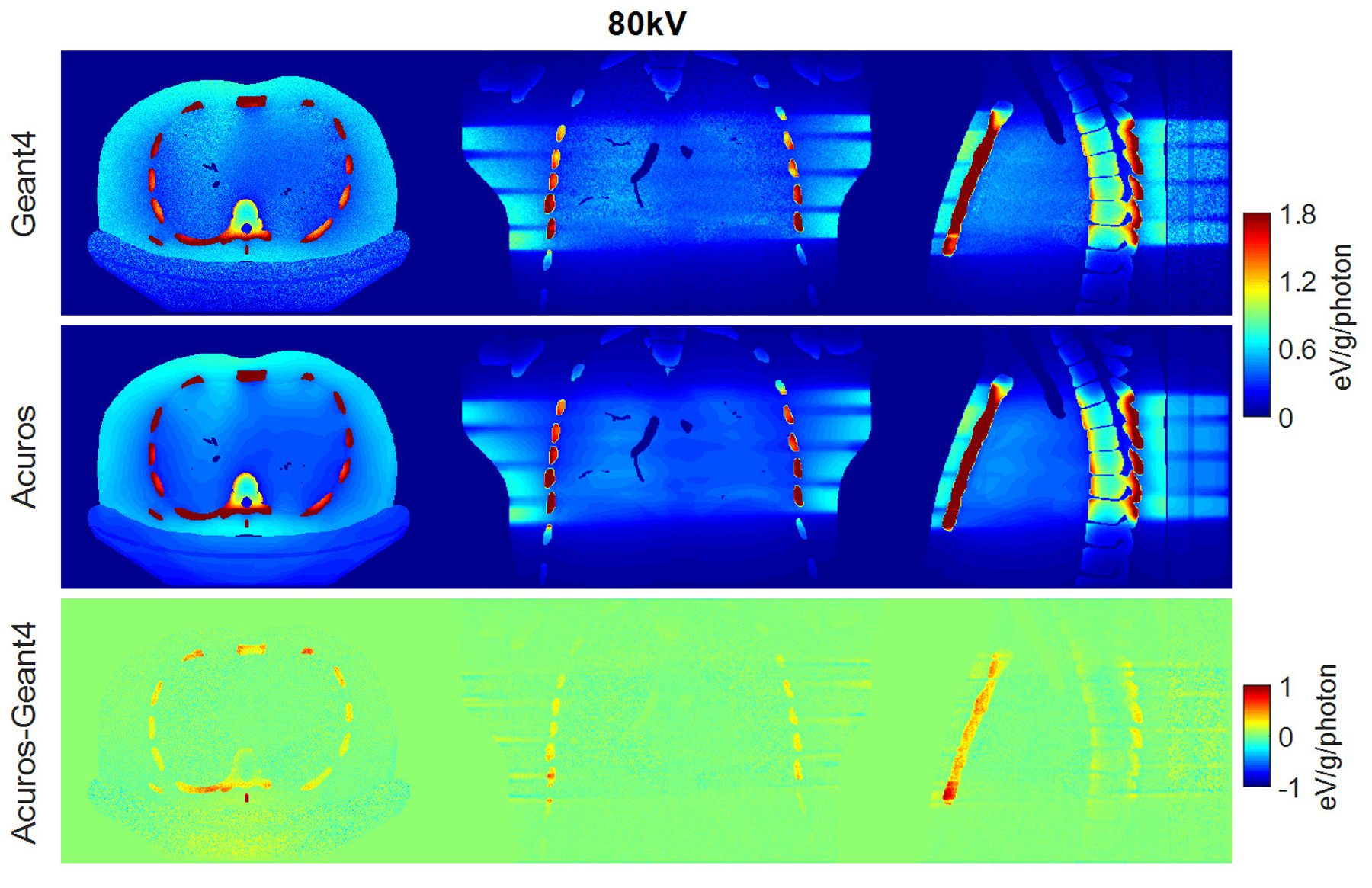
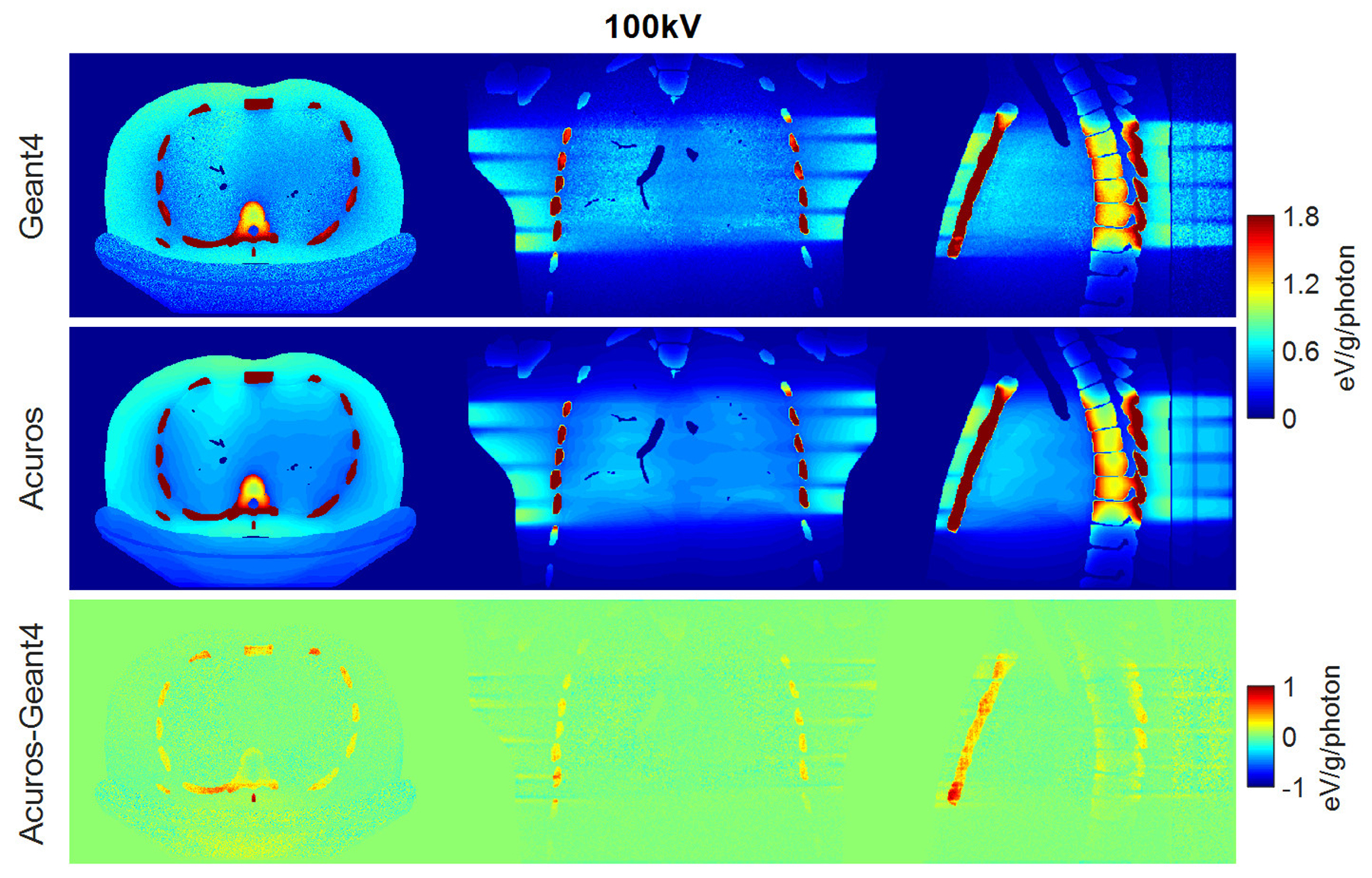
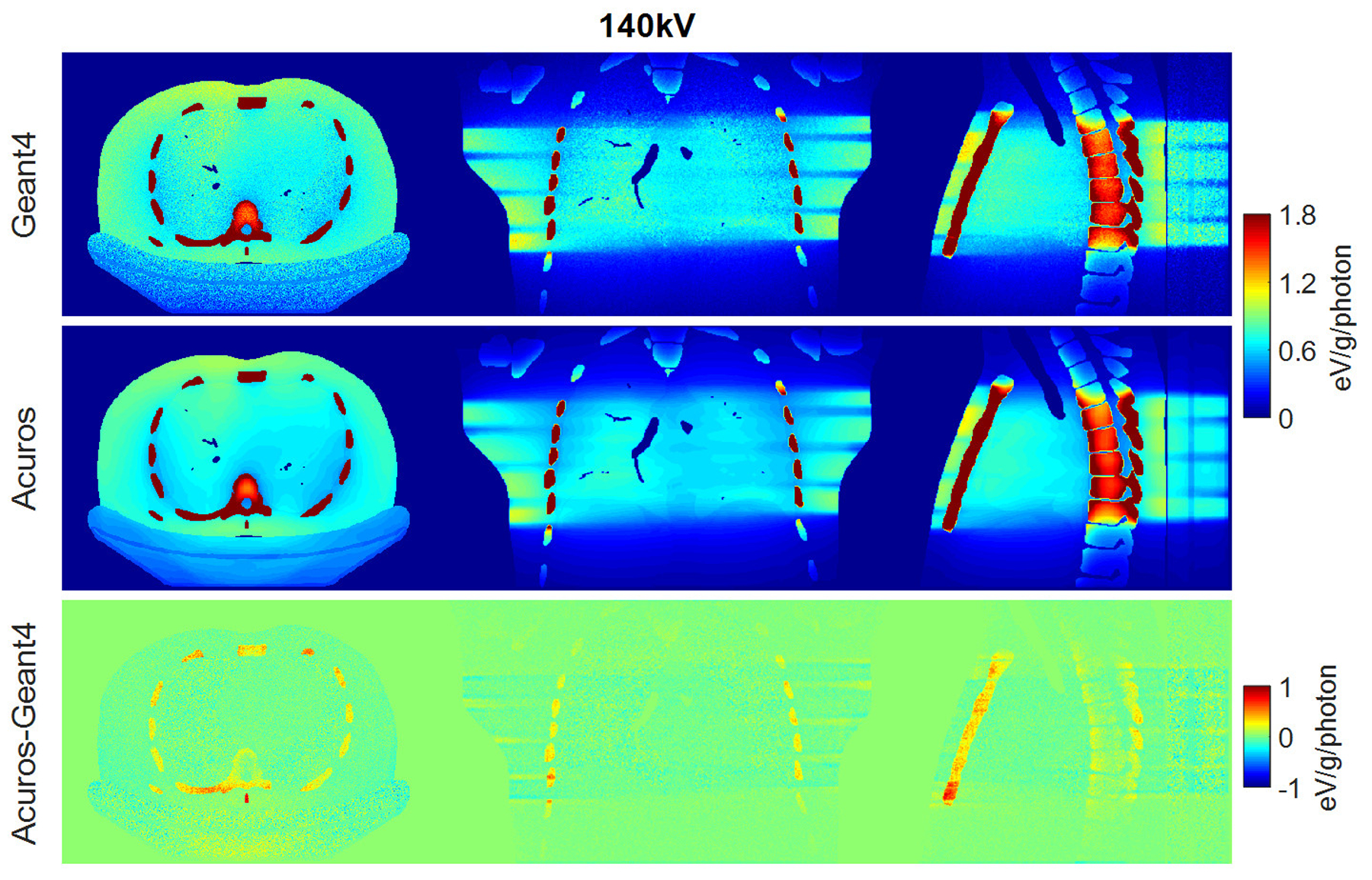
Methods: In this study, computational tools were developed for modeling CT scanners, including a bowtie filter, overrange collimation, and tube current modulation. The LBTE solver requires discretization in the spatial, angular, and spectral dimensions, which may affect the accuracy of scanner modeling. To investigate these effects, this study evaluated the LBTE dose accuracy for different discretization parameters, scanner configurations, and patient models (male, female, adults, pediatric). The method used to validate the LBTE dose maps was the Monte Carlo code Geant4, which provided ground truth dose maps. LBTE simulations were implemented on a GeForce GTX 1080 graphic unit, while Geant4 was implemented on a distributed cluster of CPUs.
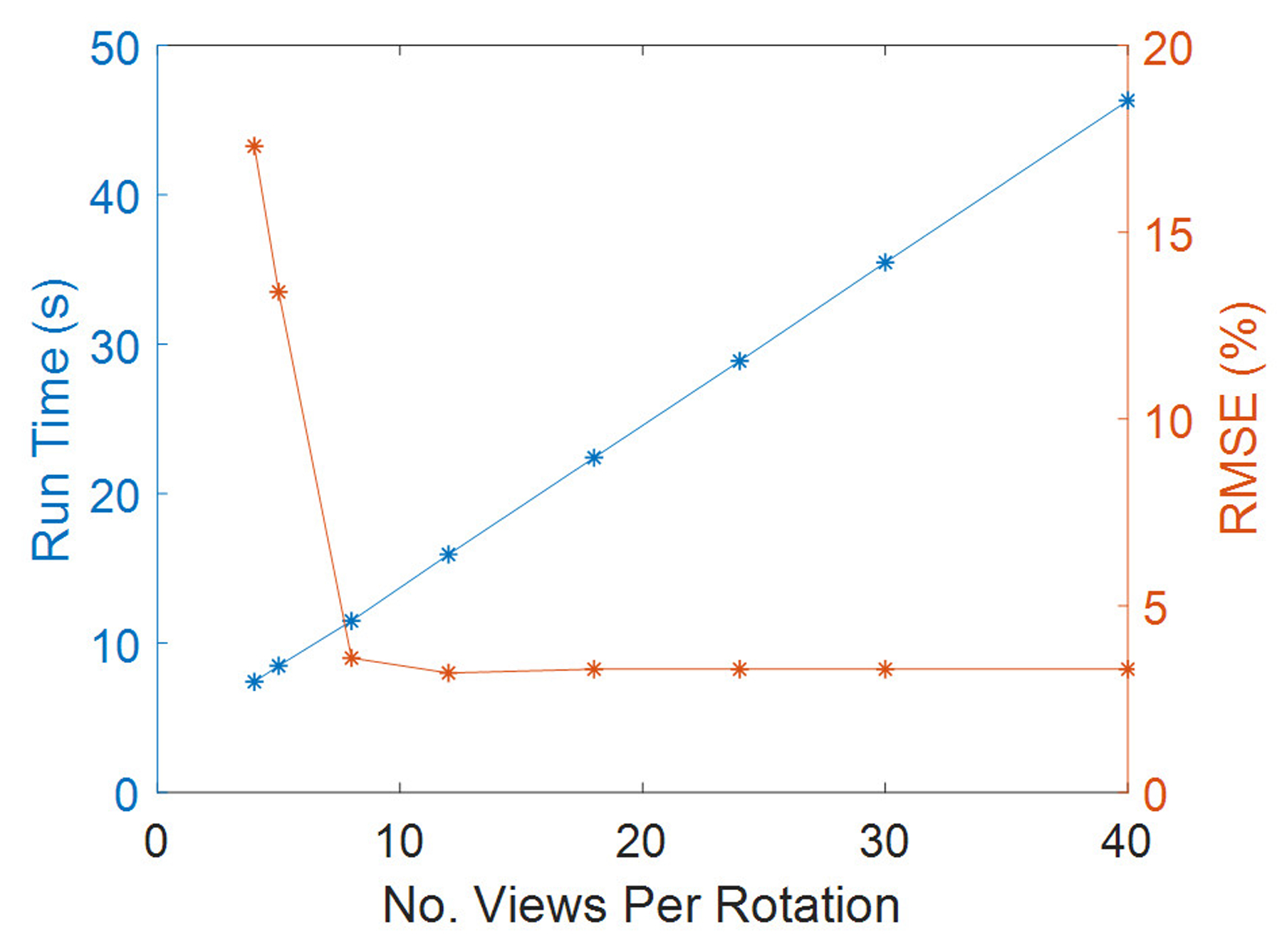
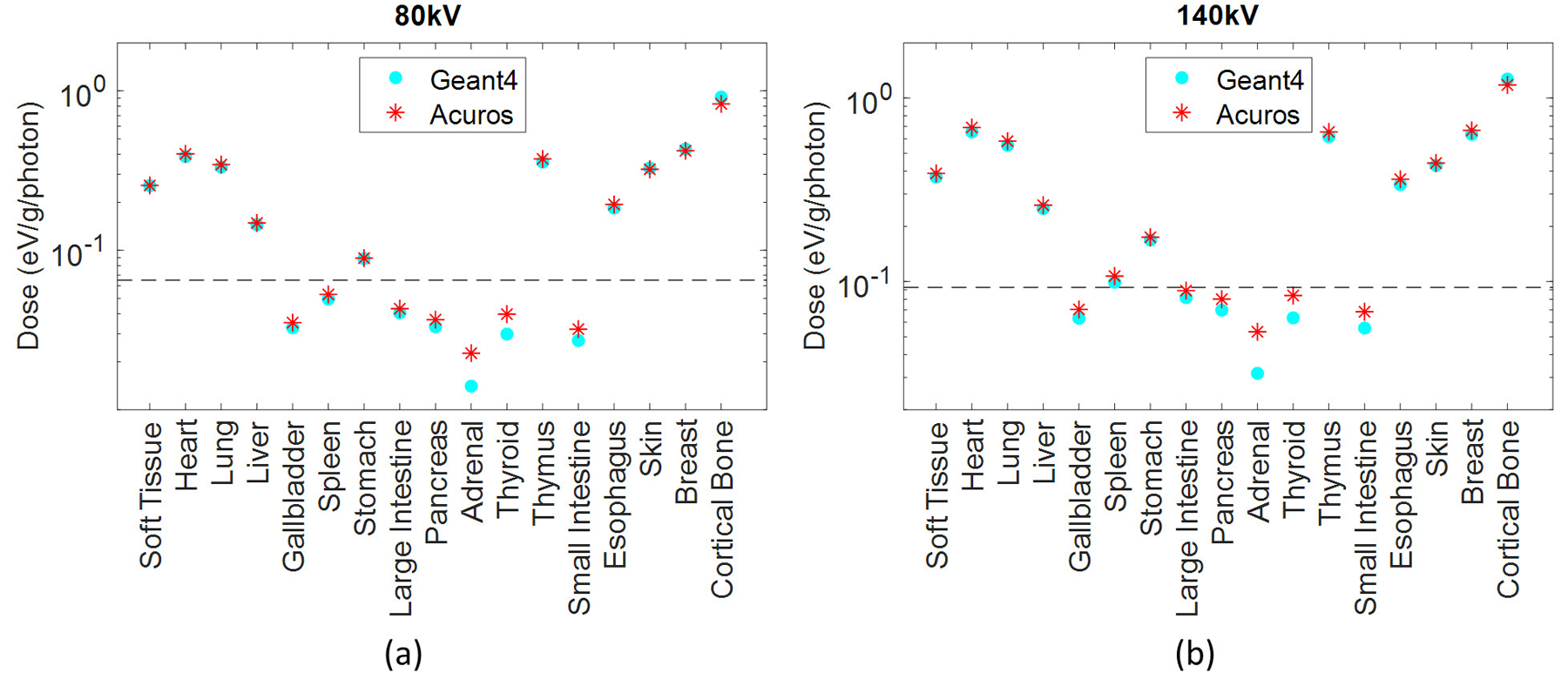
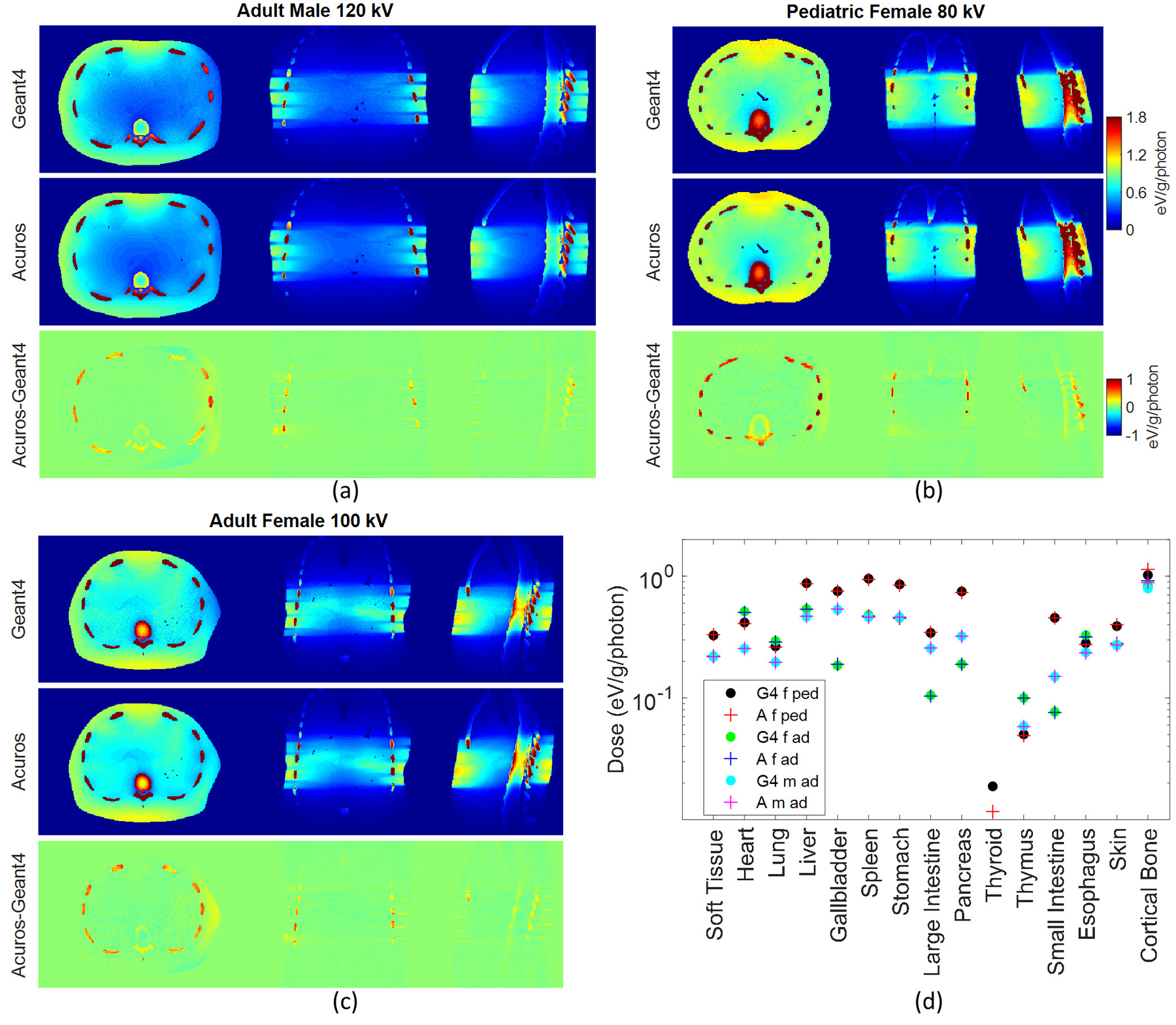
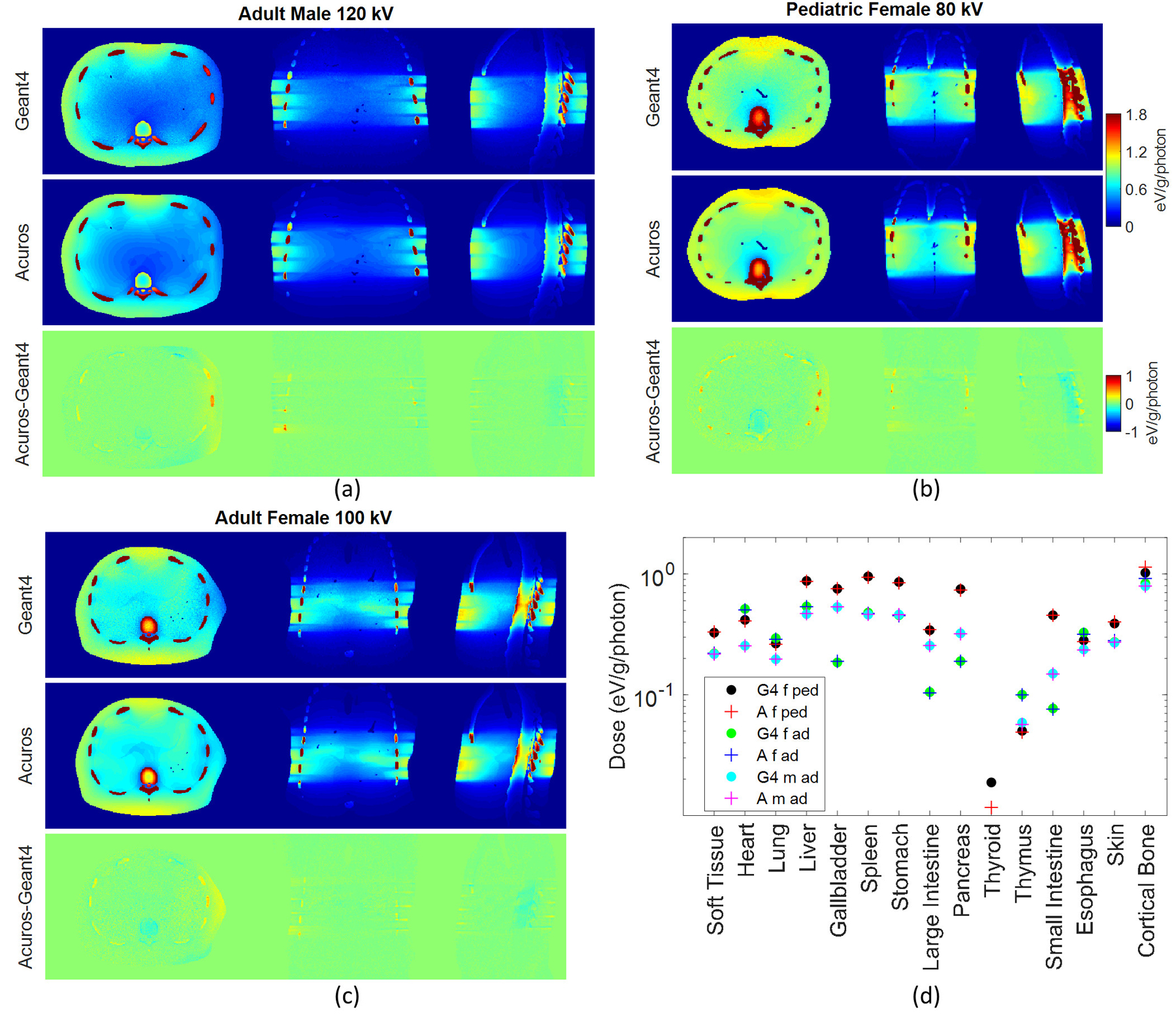
Results: The agreement between Geant4 and the LBTE solver quantifies the accuracy of the LBTE, which was similar across the different protocols and phantoms. The results suggest that 18 views per rotation provides sufficient accuracy, as no significant improvement in the accuracy was observed by increasing the number of projection views. Considering this discretization, the LBTE solver average simulation time was approximately 30 s. However, in the LBTE solver the phantom model was implemented with a lower voxel resolution with respect to Geant4, as it is limited by the memory of the GPU. Despite this discretization, the results showed a good agreement between the LBTE and Geant4, with root mean square error of the dose in organs of approximately 3.5% for most of the studied configurations.
Conclusions: The LBTE solver is proposed as an alternative to Monte Carlo for patient-specific organ dose estimation. This study demonstrated accurate organ dose estimates for the rapid LBTE solver when considering realistic aspects of CT scanners and a range of phantom models. Future plans will combine the LBTE framework with deep learning autosegmentation algorithms to provide near real-time patient-specific organ dose estimation.
Keywords: CT organ dose; Monte Carlo; deterministic solver.
© 2020 American Association of Physicists in Medicine.
Figures
References
-
- Brenner DJ, Elliston CD, Hall EJ, Berdon WE. Estimated Risks of Radiation-. Am Roentgen Ray Soc. 2001;176(February):289–296 - PubMed
-
- Tepper SJ. Computed tomography - An increasing source of radiation exposure: Commentary. Headache. 2008;48(4):657. doi:10.1111/j.1526-4610.2008.01071.x - DOI
-
- Boone JM, Hendee WR, McNitt-Gray MF, Seltzer SE. Radiation exposure from CT scans: How to close our knowledge gaps, monitor and safeguard exposure - Proceedings and recommendations of the radiation dose summit, sponsored by NIBIB, February 24–25, 2011. Radiology. 2012;265(2):544–554. doi:10.1148/radiol.12112201 - DOI - PMC - PubMed
