

Ultrasound-Guided Unilateral Transversus Abdominis Plane Combined with Rectus Sheath Block versus Subarachnoid Anesthesia in Patients Undergoing Peritoneal Dialysis Catheter Surgery: A Randomized Prospective Controlled Trial
- PMID: 32982391
- PMCID: PMC7500835
- DOI: 10.2147/JPR.S264255
Ultrasound-Guided Unilateral Transversus Abdominis Plane Combined with Rectus Sheath Block versus Subarachnoid Anesthesia in Patients Undergoing Peritoneal Dialysis Catheter Surgery: A Randomized Prospective Controlled Trial
Abstract
Background: Peritoneal dialysis catheter placement can be performed under general anesthesia, local anesthesia or subarachnoid anesthesia (SA). Recently, studies have reported the successful placement of peritoneal dialysis catheters using a transversus abdominis plane (TAP) block and rectus sheath (RS) block. This study compared the TAP + RS block with SA for patients undergoing peritoneal dialysis catheter placement.
Methods: Sixty patients were randomly divided into two groups, with 30 receiving unilateral ultrasound-guided TAP + RS block anesthesia and 30 receiving SA. The demographic characteristics, anesthesia efficacy, indicators related to anesthesia or operation, hemodynamic index, postoperative pain numeric rating score (NRS), postoperative recovery indicators, complications related to anesthesia or surgery, and dosage of sedative or analgesic medication were analyzed.
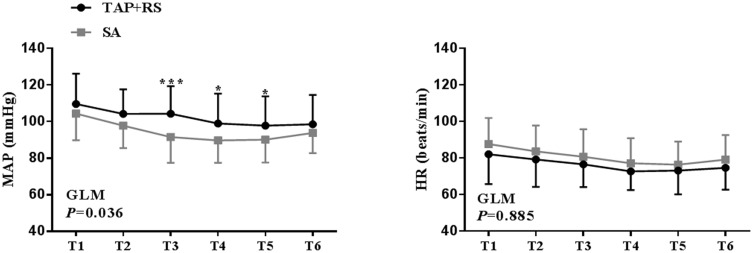
Results: Anesthesia operation time was significantly shorter in the TAP + RS block group than in the SA group (P<0.001), while there was no significant difference in success rates (TAP + RS 93.33% [95% confidence interval, 95% CI, 83.9-102.8%] vs SA 100.00% [95% CI, 100-100%], P=0.472). Two patients in the TAP + RS group needed extra analgesia, although the dermatome pinprick sensation test gave negative results for all patients. Patients who received the TAP + RS block expressed significantly less pain on movement or at rest at 4 h and 8 h postoperative. Fewer patients needed rescue analgesia with tramadol in the postoperative period in the TAP + RS block group than in the SA group (P<0.05). The intraoperative MAP was more stable (P<0.05) in the TAP + RS group compared to the SA group.
Conclusion: The TAP + RS block is a safe, effective method for use as the principal anesthesia technique in PD catheter placement. Compared to SA, it has the advantages of less influence on hemodynamics and a better postoperative analgesic effect.
Keywords: TAP block; local anesthesia; peritoneal dialysis catheter placement; rectus sheath block; subarachnoid anesthesia.
© 2020 Li et al.
Conflict of interest statement
The authors report no conflicts of interest for this work.
Figures





References
-
- CKD in the United States. An overview of USRDS annual data report volume2. ESRD: United States renal data system. Available from: http://www.usrds.org/reference.aspx. Accessed December31, 2019.
LinkOut - more resources
Full Text Sources
Miscellaneous
