

Multiple Sclerosis as a Syndrome-Implications for Future Management
- PMID: 32982904
- PMCID: PMC7483755
- DOI: 10.3389/fneur.2020.00784
Multiple Sclerosis as a Syndrome-Implications for Future Management
Abstract
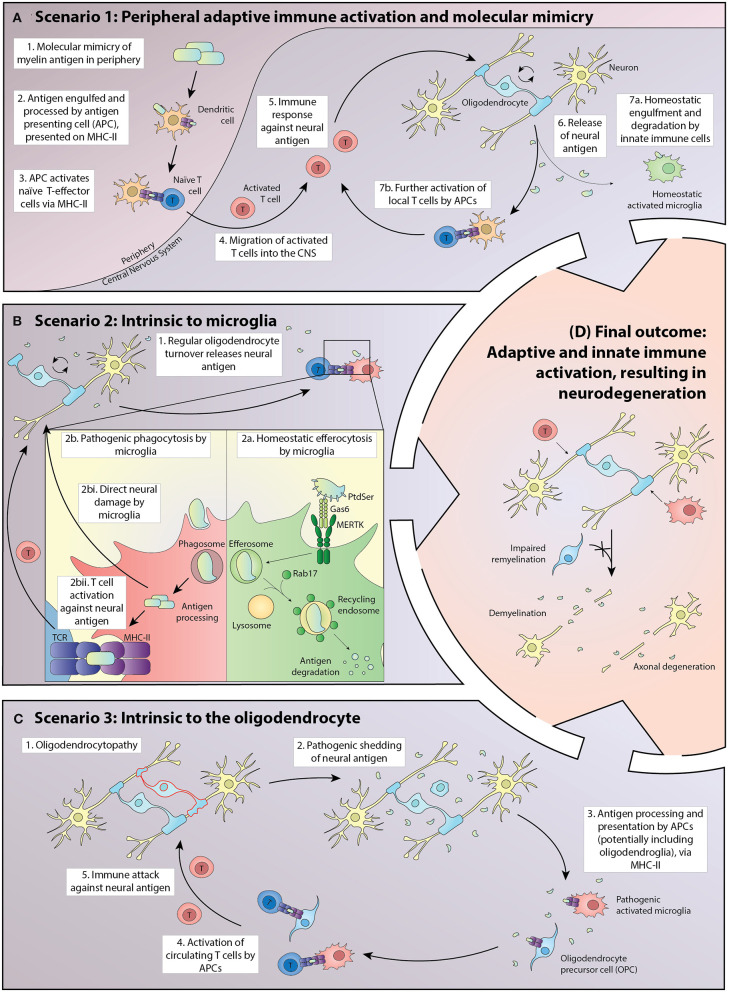
We propose that multiple sclerosis (MS) is best characterized as a syndrome rather than a single disease because different pathogenetic mechanisms can result in the constellation of symptoms and signs by which MS is clinically characterized. We describe several cellular mechanisms that could generate inflammatory demyelination through disruption of homeostatic interactions between immune and neural cells. We illustrate that genomics is important in identifying phenocopies, in particular for primary progressive MS. We posit that molecular profiling, rather than traditional clinical phenotyping, will facilitate meaningful patient stratification, as illustrated by interactions between HLA and a regulator of homeostatic phagocytosis, MERTK. We envisage a personalized approach to MS management where genetic, molecular, and cellular information guides management.
Keywords: demyelination; innate immunity; multiple sclerosis; pathophysiology; syndrome.
Copyright © 2020 Dwyer, Nguyen, Healy, Dutta, Ludwin, Antel, Binder and Kilpatrick.
Figures
References
-
- Compston McAlpine's Multiple Sclerosis. Philadelphia, PA: Churchill Livingstone Elsevier; (2005).
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous