

Effect of Combined Therapy of Virtual Reality and Transcranial Direct Current Stimulation in Children and Adolescents With Cerebral Palsy: A Study Protocol for a Triple-Blinded Randomized Controlled Crossover Trial
- PMID: 32982950
- PMCID: PMC7492207
- DOI: 10.3389/fneur.2020.00953
Effect of Combined Therapy of Virtual Reality and Transcranial Direct Current Stimulation in Children and Adolescents With Cerebral Palsy: A Study Protocol for a Triple-Blinded Randomized Controlled Crossover Trial
Abstract
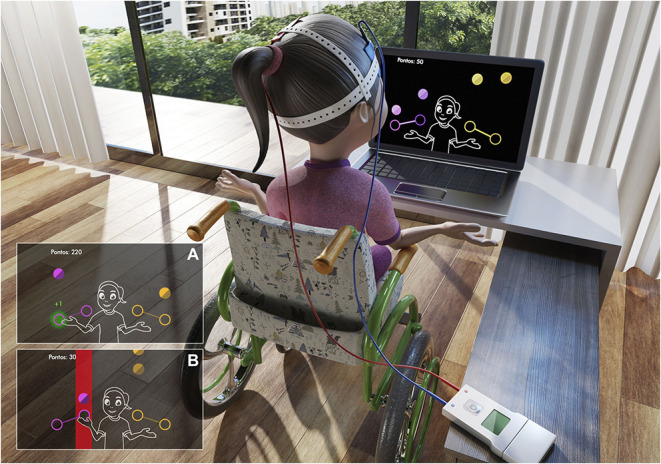
Background: Transcranial direct current stimulation (tDCS) and therapy-based virtual reality (VR) have been investigated separately. They have shown promise as efficient and engaging new tools in the neurological rehabilitation of individuals with cerebral palsy (CP). However, the recent literature encourages investigation of the combination of therapy tools in order to potentiate clinic effects and its mechanisms. Methods: A triple-blinded randomised sham-controlled crossover trial will be performed. Thirty-six individuals with gross motor function of levels I to IV (aged 4-14 years old) will be recruited. Individuals will be randomly assigned to Group A (active first) or S (sham first): Group A will start with ten sessions of active tDSC combined with VR tasks. After a 1-month washout, this group will be reallocated to another ten sessions with sham tDCS combined with VR tasks. In contrast, Group S will carry out the opposite protocol, starting with sham tDCS. For the active tDCS the protocol will use low frequency tDCS [intensity of 1 milliampere (mA)] over the primary cortex (M1) area on the dominant side of the brain. Clinical evaluations (reaction times and coincident timing through VR, functional scales: Abilhand-Kids, ACTIVLIM-CP, Paediatric Evaluation of Disability Inventory-PEDI- and heart rate variability-HRV) will be performed at baseline, during, and after active and sham tDCS. Conclusion: tDCS has produced positive results in treating individuals with CP; thus, its combination with new technologies shows promise as a potential mechanism for improving neurological functioning. The results of this study may provide new insights into motor rehabilitation, thereby contributing to the better use of combined tDCS and VR in people with CP. Trial Registration: ClinicalTrials.gov, NCT04044677. Registered on 05 August 2019.
Keywords: autonomic nervous system; cerebral palsy; motor rehabilitation; non-invasive brain stimulation; plasticity; transcranial direct current stimulation; virtual reality exposure therapy.
Copyright © 2020 Silva, Fontes, Oliveira-Furlan, Roque, Lima, Souza, Alberissi, Silveira, Moraes, Collett, Silva, Airoldi, Ribeiro-Papa, Dawes and Monteiro.
Figures





References
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous