

Coagulation and Fibrinolysis in Kidney Graft Rejection
- PMID: 32983089
- PMCID: PMC7477357
- DOI: 10.3389/fimmu.2020.01807
Coagulation and Fibrinolysis in Kidney Graft Rejection
Abstract
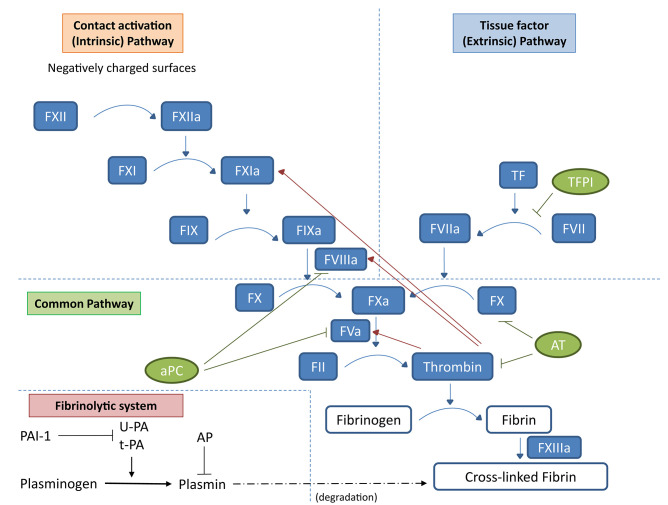
Coagulation system is currently considered an integrated part of innate immunity. Clotting activation in response to bacterial surface along with complement cascade priming represents the first line of defense against pathogens. In the last three decades, we learned that several coagulation factors, including factor II or thrombin and factor X, can interact with specific cell surface receptors activated by an unusual proteolytic mechanism and belonging to a novel class of G-protein-coupled receptors known as protease-activated receptors (PARs). PARs are expressed by a variety of cells, including monocytes, dendritic cells, and endothelial cells and may play a key role in the modulation of innate immunity and in the regulation of its interaction with the adaptive branch of the immune system. Also, the fibrinolytic system, in which activation is controlled by coagulation, can interact with innate immunity, and it is a key modulator of extracellular matrix deposition eventually leading to scarring and fibrosis. In the setting of kidney transplantation, coagulation and fibrinolytic systems have been shown to play key roles in the ischemia/reperfusion injury featuring delayed graft function and in the pathogenesis of tissue damage following acute and chronic rejection. In the present review, we aim to describe the mechanisms leading to coagulation and fibrinolysis activation in this setting and their interaction with the priming of the innate immune response and their role in kidney graft rejection.
Keywords: coagulation; fibrinolysis; graft function; innate immunity; protease-activated receptors.
Copyright © 2020 Stallone, Pontrelli, Rascio, Castellano, Gesualdo and Grandaliano.
Figures
Similar articles
-
Editorial: Kidney Transplantation and Innate Immunity.Front Immunol. 2020 Oct 14;11:603982. doi: 10.3389/fimmu.2020.603982. eCollection 2020. Front Immunol. 2020. PMID: 33154759 Free PMC article. No abstract available.
-
Effects of Antirejection Drugs on Innate Immune Cells After Kidney Transplantation.Front Immunol. 2019 Dec 19;10:2978. doi: 10.3389/fimmu.2019.02978. eCollection 2019. Front Immunol. 2019. PMID: 31921213 Free PMC article. Review.
-
Coagulation, protease-activated receptors, and viral myocarditis.J Cardiovasc Transl Res. 2014 Mar;7(2):203-11. doi: 10.1007/s12265-013-9515-7. Epub 2013 Nov 8. J Cardiovasc Transl Res. 2014. PMID: 24203054 Free PMC article. Review.
-
Proteinase-activated receptors (PARs): crossroads between innate immunity and coagulation.Curr Opin Pharmacol. 2006 Aug;6(4):428-34. doi: 10.1016/j.coph.2006.05.001. Epub 2006 Jun 13. Curr Opin Pharmacol. 2006. PMID: 16777485 Review.
-
Protease-activated receptor 1 and plasminogen activator inhibitor 1 expression in chronic allograft nephropathy: the role of coagulation and fibrinolysis in renal graft fibrosis.Transplantation. 2001 Oct 27;72(8):1437-43. doi: 10.1097/00007890-200110270-00018. Transplantation. 2001. PMID: 11685117
Cited by
-
A Review of the Risk Factors and Approaches to Prevention of Post-Reperfusion Syndrome During Liver Transplantation.Organogenesis. 2024 Dec 31;20(1):2386730. doi: 10.1080/15476278.2024.2386730. Epub 2024 Aug 4. Organogenesis. 2024. PMID: 39097866 Free PMC article. Review.
-
Establishment and analysis of an animal model for nutcracker syndrome.Int Urol Nephrol. 2025 Feb;57(2):419-426. doi: 10.1007/s11255-024-04245-9. Epub 2024 Oct 18. Int Urol Nephrol. 2025. PMID: 39422826
-
Dendritic Cells: Versatile Players in Renal Transplantation.Front Immunol. 2021 May 19;12:654540. doi: 10.3389/fimmu.2021.654540. eCollection 2021. Front Immunol. 2021. PMID: 34093544 Free PMC article. Review.
-
Cardiovascular Risk after Kidney Transplantation: Causes and Current Approaches to a Relevant Burden.J Pers Med. 2022 Jul 23;12(8):1200. doi: 10.3390/jpm12081200. J Pers Med. 2022. PMID: 35893294 Free PMC article. Review.
-
Shedding light on the molecular and regulatory mechanisms of TLR4 signaling in endothelial cells under physiological and inflamed conditions.Front Immunol. 2023 Nov 24;14:1264889. doi: 10.3389/fimmu.2023.1264889. eCollection 2023. Front Immunol. 2023. PMID: 38077393 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous