

Case Reports
doi: 10.1002/ccr3.2935.
eCollection 2020 Sep.
Presentation and resolution of gender dysphoria as a positive symptom in a young schizophrenic man who presented with self-emasculation: Frontiers of bioethics, psychiatry, and microsurgical genital reconstruction
Affiliations
- PMID: 32983487
- PMCID: PMC7495809
- DOI: 10.1002/ccr3.2935
Item in Clipboard
Case Reports
Presentation and resolution of gender dysphoria as a positive symptom in a young schizophrenic man who presented with self-emasculation: Frontiers of bioethics, psychiatry, and microsurgical genital reconstruction
Clin Case Rep.
.
Abstract
Gender dysphoria can present as a positive symptom of schizophrenia. Completion of gender affirmation surgeries should not occur as a result of male genital self-mutilation via a deferral of emergent surgical reconstruction. Instead, gender affirmation should be considered after a full workup and assessment for resolution of any acute psychosis.
Keywords: gender dysphoria; penis; schizophrenia; self‐amputation; self‐castration.
© 2020 The Authors. Clinical Case Reports published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors report no competing interests.
Figures
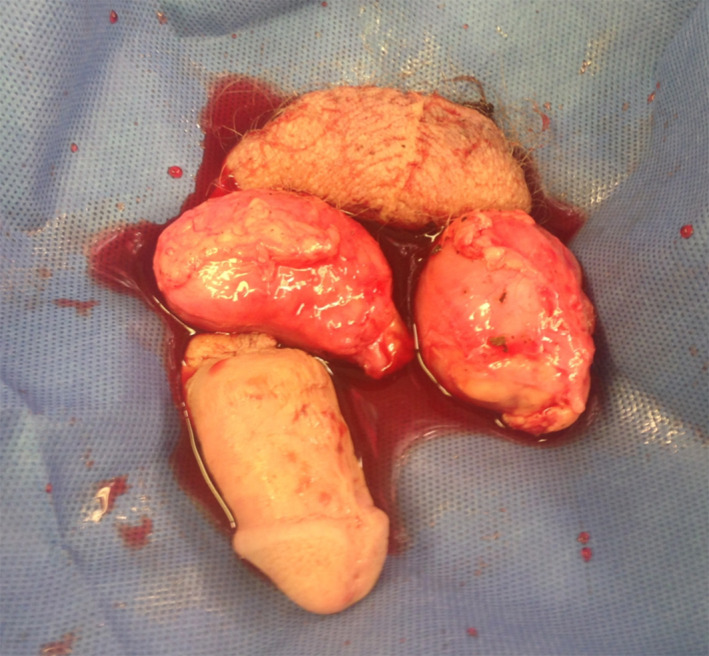
Amputated penis, testicles, and scrotum. Distal penile stump was approximately 5 cm in length. Bilateral testes were amputated near the epididymides with approximately 3‐4 mm of spermatic cord stump remaining on the testicular side
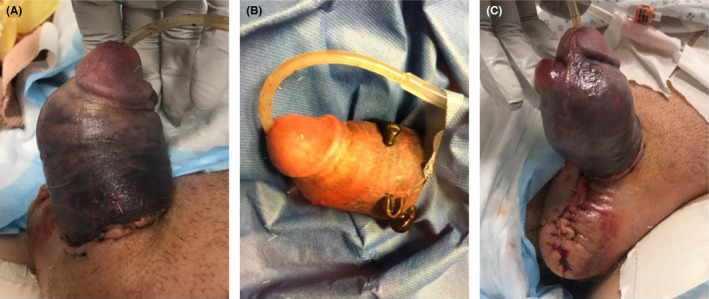
Medical leech therapy. A, Ecchymosis and hematoma as seen before initiation of therapy. B, Initial response to therapy. C, Development of necrosis with bullae
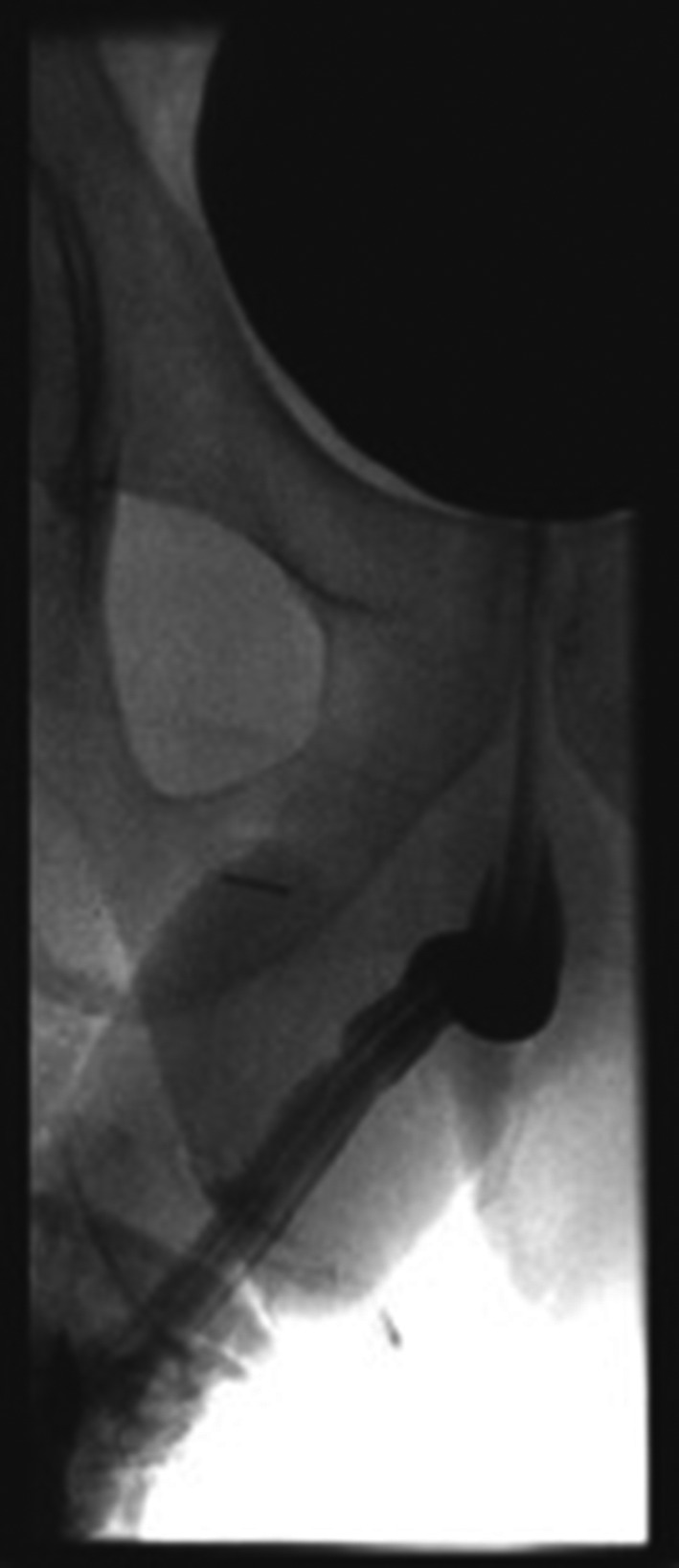
Retrograde Urethrogram. No evidence of stricture or extravasation
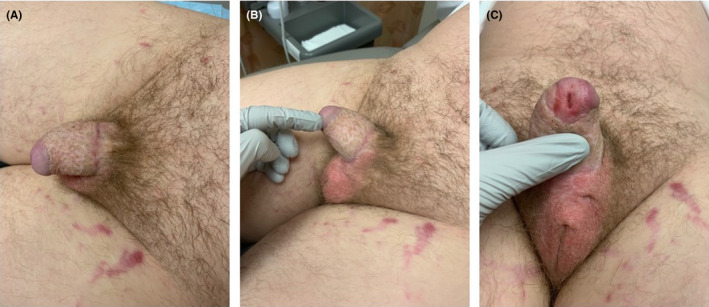
Penis at 1‐y follow up visit. A, Dorsal view, (B) left lateral view, (C) ventral view with patent meatus and scrotum
Similar articles
-
Self-emasculation and self-castration: immediate surgical management and ultimate psychological adjustment.J Urol. 1980 Aug;124(2):208-9. doi: 10.1016/s0022-5347(17)55375-6. J Urol. 1980. PMID: 7401234
-
The Intersection of Gender Dysphoria and Psychosis: Case Report of a Patient With Schizophrenia, Gender Dysphoria, and Repeated Genital Self-Mutilation.J Acad Consult Liaison Psychiatry. 2023 Sep-Oct;64(5):482-483. doi: 10.1016/j.jaclp.2023.04.004. J Acad Consult Liaison Psychiatry. 2023. PMID: 37689461 No abstract available.
-
Successful microsurgical penile replantation following self amputation in a schizophrenic patient.Indian J Urol. 2010 Jul;26(3):434-7. doi: 10.4103/0970-1591.70589. Indian J Urol. 2010. Retraction in: Indian J Urol. 2013 Jul;29(3):172. PMID: 21116370 Free PMC article. Retracted.
-
Gender-Affirming Penile Inversion Vaginoplasty.Clin Plast Surg. 2018 Jul;45(3):343-350. doi: 10.1016/j.cps.2018.04.001. Clin Plast Surg. 2018. PMID: 29908622 Review.
-
Male-to-female gender affirmation surgery: breast reconstruction with Ergonomix round prostheses.Int J Impot Res. 2020 Nov;33(7):720-725. doi: 10.1038/s41443-021-00425-8. Epub 2021 Mar 15. Int J Impot Res. 2020. PMID: 33723376 Review.
Cited by
-
A fatal and unusual genital mutilation in an elderly man as a result of sharp force injuries and domestic dog predation.Forensic Sci Med Pathol. 2023 Sep;19(3):398-402. doi: 10.1007/s12024-022-00542-w. Epub 2022 Oct 14. Forensic Sci Med Pathol. 2023. PMID: 36239912 Free PMC article.
-
Sexual and Reproductive Health in Adolescents and Young Adults With Psychotic Disorders: A Scoping Review.Schizophr Bull. 2023 Jan 3;49(1):108-135. doi: 10.1093/schbul/sbac114. Schizophr Bull. 2023. PMID: 36065153 Free PMC article.
References
-
- Doyle D. Ritual male circumcision: a brief history. J R Coll Physicians Edinb. 2005;35:279–285. - PubMed
-
- Zislin J, Katz G, Raskin S, Strauss Z, Teitelbaum A, Durst R. Male genital self‐mutilation in the context of religious belief: the Jerusalem syndrome. Transcult Psychiatry. 2002;39(2):257‐264.
-
- Jezior JR, Brady JD, Schlossberg SM. Management of penile amputation injuries. World J Surg. 2001;25(12):1602‐1609. - PubMed
-
- Veeder TA, Leo RJ. Male genital self‐mutilation: a systematic review of psychiatric disorders and psychosocial factors. Gen Hosp Psychiatry. 2017;44:43‐50. - PubMed
-
- Bhanganada K, Chayavatana T, Pongnumkul C, et al, Surgical management of an epidemic of penile amputations in siam. Am J Surg. 1983;146(3):376‐382. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
