

Encephalopathy in COVID-19 patients; viral, parainfectious, or both?
- PMID: 32984561
- PMCID: PMC7505131
- DOI: 10.1016/j.ensci.2020.100275
Encephalopathy in COVID-19 patients; viral, parainfectious, or both?
Erratum in
-
Corrigendum to 'Encephalopathy in COVID-19 patients; viral, parainfectious, or both?' [eNeurologicalScic(Volume 21), December 2020, 100275].eNeurologicalSci. 2021 Jun;23:100336. doi: 10.1016/j.ensci.2021.100336. Epub 2021 Mar 20. eNeurologicalSci. 2021. PMID: 33778176 Free PMC article.
-
Corrigendum to "Encephalopathy in COVID-19 patients; viral, parainfectious, or both?" [eNeurologicalScic(Volume 21), December 2020, 100275].eNeurologicalSci. 2021 Dec;25:100373. doi: 10.1016/j.ensci.2021.100373. Epub 2021 Oct 28. eNeurologicalSci. 2021. PMID: 34729425 Free PMC article.
Abstract
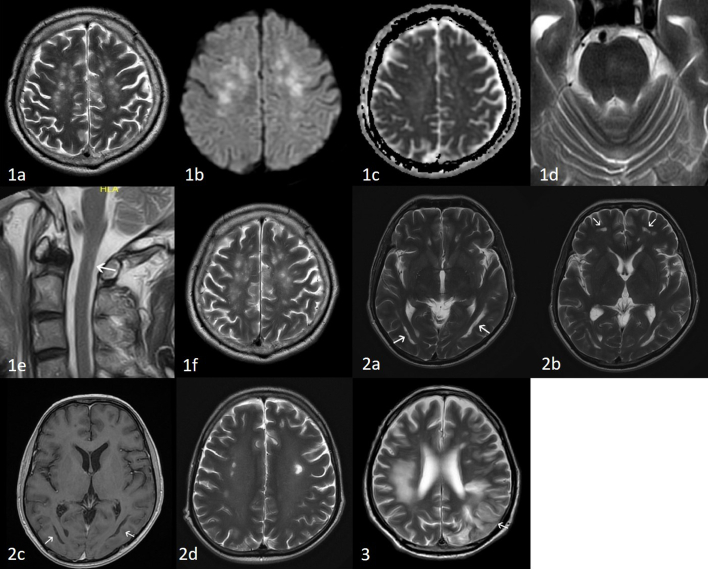
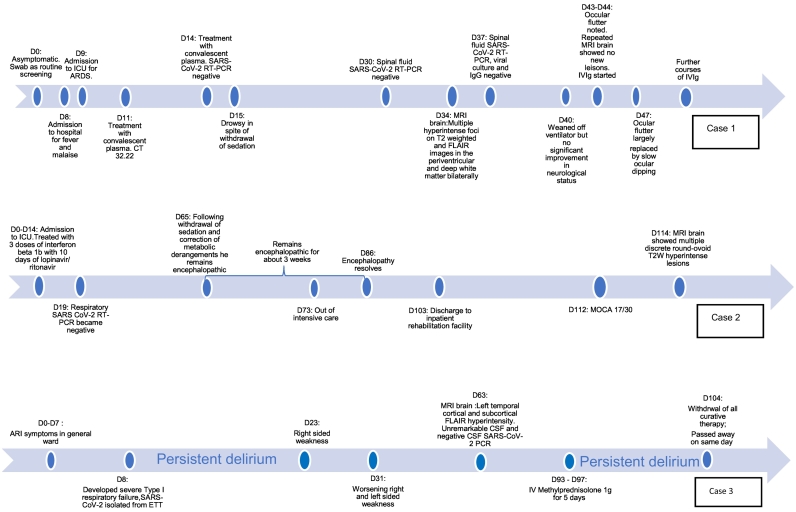
We describe the clinical, laboratory and radiological features of 3 critically ill patients with COVID-19 who developed severe encephalopathy. The first patient did not regain consciousness when sedation was removed at the end of 2 weeks of intensive care. He had received treatment with convalescent plasma. His clinical examination was remarkable for intact brainstem reflexes, roving eye movements, later transient ocular flutter; and then what appeared to be slow ocular dipping. He had no coherent volitional response to the environment. The second patient recovered with measurable cognitive deficits after a prolonged period of encephalopathy. He had received combination treatment with interferon beta 1b and lopinavir/ritonavir. The third patient remained in persistent, severe agitated delirium and died 3 months into his illness. The MRI of the 3 patients showed multifocal abnormalities predominantly in the cerebral white matter, with varying involvement of the grey matter, brainstem and spinal cord. Case 1's MRI changes were consistent with acute disseminated encephalomyelitis. The patients also displayed blood markers, to varying degree, of autoimmunity and hypercoagulability. We were not able to convincingly show, from microbiological as well as immunological evaluation, if the effects of COVID-19 on these patients' nervous system were a direct consequence of the virus, proinflammatory-thrombotic state or a combination. Patient 1 responded partially to empirical, albeit delayed, therapy with intravenous immunoglobulins. Patient 2 recovered with no specific treatment. These cases illustrate the need to understand the full spectrum of encephalopathy associated with COVID-19 so as to better guide its management.
Keywords: Autoimmunity; COVID-19; Encephalitis; Parainfectious; SARS-CoV-2 virus.
© 2020 The Author(s).
Figures
References
-
- Hung E.C.W., Chim S.S.C., Chan P.K.S., Tong Y.K., Ng E.K.O., Chiu R.W.K., Leung C.-B., Sung J.J.Y., Tam J.S., Lo Y.M.D. Detection of SARS coronavirus RNA in the cerebrospinal fluid of a patient with severe acute respiratory syndrome. Clin. Chem. 2003;49:2108–2109. doi: 10.1373/clinchem.2003.025437. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
