

A rare case of corneal keloid occurred 30 years after pterygium surgery and 3 years after cataract surgery
- PMID: 32984646
- PMCID: PMC7494458
- DOI: 10.1016/j.ajoc.2020.100901
A rare case of corneal keloid occurred 30 years after pterygium surgery and 3 years after cataract surgery
Abstract
Purpose: We report a case of corneal keloid occurring 30 years after pterygium surgery and 3 years after cataract surgery.
Observations: The case of a 72-year-old man was referred because of blurred vision and corneal opacity in the right eye. Pterygium surgery had been performed on the right eye 30 years earlier, and bilateral cataract surgery had been done uneventfully via a temporal corneal incision 3 years ago. Deterioration of vision occurred in the right eye from 2 years ago. At the initial visit, his best corrected visual acuity (BCVA) was 20/2000 on the right. A white nodule that was well demarcated from the underlying stroma was seen on the right cornea. The nodule was excised by superficial keratectomy, with BCVA being 180/200 at 1 week after surgery. Pathological examination of the resected specimen revealed proliferation of fibroblasts and haphazard arrangement of collagen bundles, leading to a diagnosis of corneal keloid. Keloid-like lesion was also later noted in temporal corneal incision site of cataract surgery.
Conclusions and importance: This rare case of corneal keloid occurred as a late complication of pterygium surgery.
Keywords: Corneal keloid; Pterygium surgery; Superficial keratectomy.
© 2020 Published by Elsevier Inc.
Conflict of interest statement
None.
Figures

- (A)
A year after the cataract surgery, corneal opacification located around the pupil zone of right eye was noted at the visit of the local clinic.
- (B)
At the initial visit of our hospital, slit-lamp microscopy identified a pearly white, elevated lesion with a smooth surface on the central right cornea.
- (C)
The left cornea was clear.
- (D)
Anterior segment optical coherence tomography (OCT) demonstrated well-demarcated lesions in the subepithelial region and anterior corneal stroma, with clear underlying posterior stroma, as well as a continuous high-intensity subepithelial lesion located around the main lesion and extending inferiorly toward the nasal limbus.
- (E)
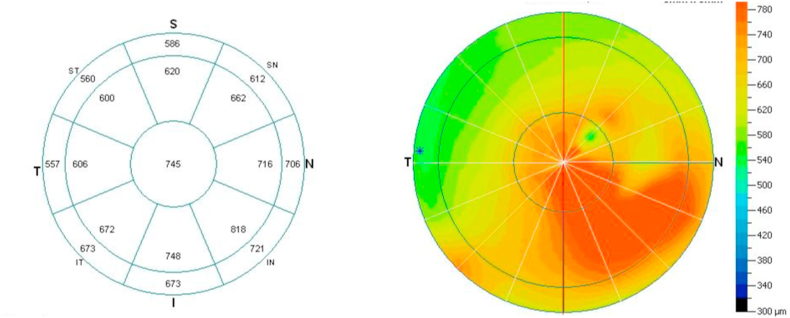
Measurement of corneal thickness by anterior segment OCT revealed thickening of the cornea from the center to the inferior nasal region.

- (A)
A year after the cataract surgery, corneal opacification located around the pupil zone of right eye was noted at the visit of the local clinic.
- (B)
At the initial visit of our hospital, slit-lamp microscopy identified a pearly white, elevated lesion with a smooth surface on the central right cornea.
- (C)
The left cornea was clear.
- (D)
Anterior segment optical coherence tomography (OCT) demonstrated well-demarcated lesions in the subepithelial region and anterior corneal stroma, with clear underlying posterior stroma, as well as a continuous high-intensity subepithelial lesion located around the main lesion and extending inferiorly toward the nasal limbus.
- (E)
Measurement of corneal thickness by anterior segment OCT revealed thickening of the cornea from the center to the inferior nasal region.

- (A)
A year after the cataract surgery, corneal opacification located around the pupil zone of right eye was noted at the visit of the local clinic.
- (B)
At the initial visit of our hospital, slit-lamp microscopy identified a pearly white, elevated lesion with a smooth surface on the central right cornea.
- (C)
The left cornea was clear.
- (D)
Anterior segment optical coherence tomography (OCT) demonstrated well-demarcated lesions in the subepithelial region and anterior corneal stroma, with clear underlying posterior stroma, as well as a continuous high-intensity subepithelial lesion located around the main lesion and extending inferiorly toward the nasal limbus.
- (E)
Measurement of corneal thickness by anterior segment OCT revealed thickening of the cornea from the center to the inferior nasal region.

- (A)
A year after the cataract surgery, corneal opacification located around the pupil zone of right eye was noted at the visit of the local clinic.
- (B)
At the initial visit of our hospital, slit-lamp microscopy identified a pearly white, elevated lesion with a smooth surface on the central right cornea.
- (C)
The left cornea was clear.
- (D)
Anterior segment optical coherence tomography (OCT) demonstrated well-demarcated lesions in the subepithelial region and anterior corneal stroma, with clear underlying posterior stroma, as well as a continuous high-intensity subepithelial lesion located around the main lesion and extending inferiorly toward the nasal limbus.
- (E)
Measurement of corneal thickness by anterior segment OCT revealed thickening of the cornea from the center to the inferior nasal region.
- (A)
A year after the cataract surgery, corneal opacification located around the pupil zone of right eye was noted at the visit of the local clinic.
- (B)
At the initial visit of our hospital, slit-lamp microscopy identified a pearly white, elevated lesion with a smooth surface on the central right cornea.
- (C)
The left cornea was clear.
- (D)
Anterior segment optical coherence tomography (OCT) demonstrated well-demarcated lesions in the subepithelial region and anterior corneal stroma, with clear underlying posterior stroma, as well as a continuous high-intensity subepithelial lesion located around the main lesion and extending inferiorly toward the nasal limbus.
- (E)
Measurement of corneal thickness by anterior segment OCT revealed thickening of the cornea from the center to the inferior nasal region.
- (A)
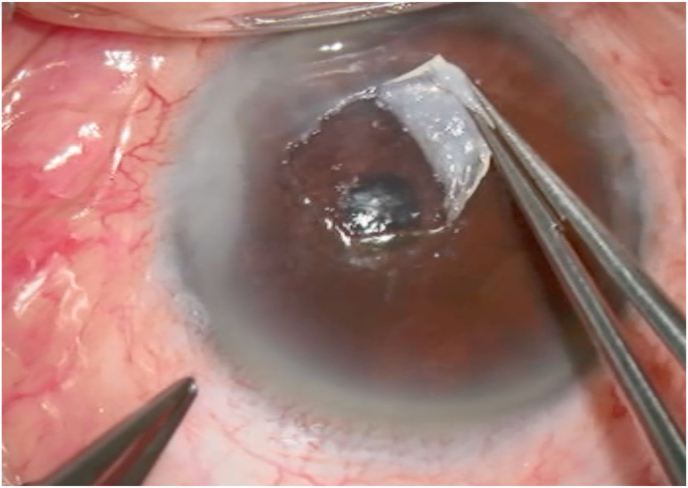
During superficial keratectomy, the central lesion was easily dissected from the corneal stroma.
- (B)
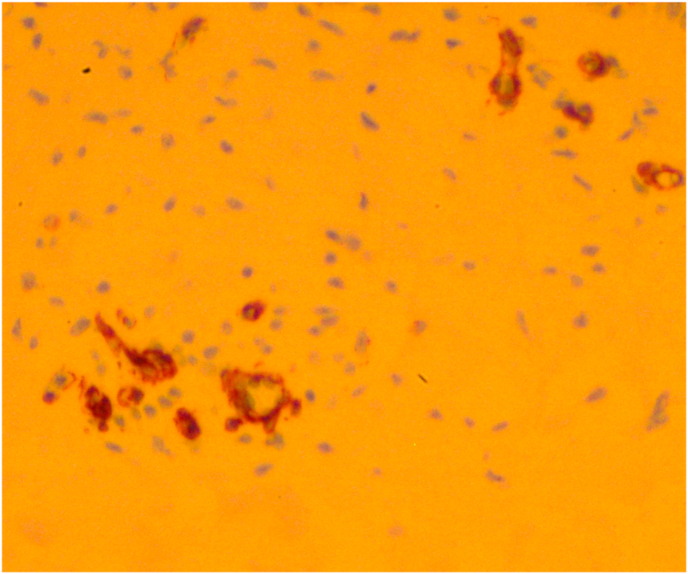
Light microscopic examination of the resected specimen revealed hyperplastic epithelium, absence of Bowman's layer, irregular collagen fibrils, and infiltration of fibroblasts, findings which were consistent with a diagnosis of corneal keloid.
- (C)
Immunohistochemistry using alpha-smooth muscle actin antibody revealed that fibroblast-like cells noted in corneal stroma were myofibroblasts.
- (A)
During superficial keratectomy, the central lesion was easily dissected from the corneal stroma.
- (B)
Light microscopic examination of the resected specimen revealed hyperplastic epithelium, absence of Bowman's layer, irregular collagen fibrils, and infiltration of fibroblasts, findings which were consistent with a diagnosis of corneal keloid.
- (C)
Immunohistochemistry using alpha-smooth muscle actin antibody revealed that fibroblast-like cells noted in corneal stroma were myofibroblasts.

- (A)
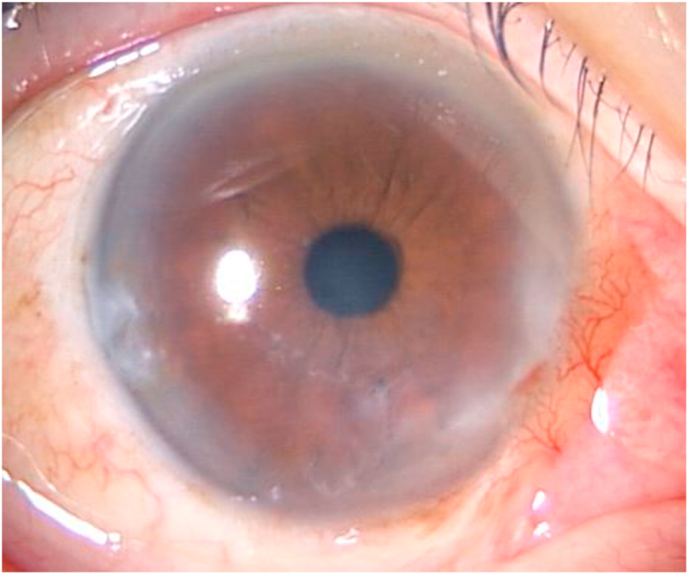
Epithelialization at 1 week after superficial keratectomy.
- (B)
A small recurrent white opacity on the inferior cornea at 6 months after superficial keratectomy.
- (C)
Worsening of pearly white lesion in temporal corneal incision site of cataract surgery 5 years ago was noted.
- (D)
While contralateral cornea remained clear.
- (A)
Epithelialization at 1 week after superficial keratectomy.
- (B)
A small recurrent white opacity on the inferior cornea at 6 months after superficial keratectomy.
- (C)
Worsening of pearly white lesion in temporal corneal incision site of cataract surgery 5 years ago was noted.
- (D)
While contralateral cornea remained clear.

- (A)
Epithelialization at 1 week after superficial keratectomy.
- (B)
A small recurrent white opacity on the inferior cornea at 6 months after superficial keratectomy.
- (C)
Worsening of pearly white lesion in temporal corneal incision site of cataract surgery 5 years ago was noted.
- (D)
While contralateral cornea remained clear.

- (A)
Epithelialization at 1 week after superficial keratectomy.
- (B)
A small recurrent white opacity on the inferior cornea at 6 months after superficial keratectomy.
- (C)
Worsening of pearly white lesion in temporal corneal incision site of cataract surgery 5 years ago was noted.
- (D)
While contralateral cornea remained clear.
References
-
- Vanathi M., Panda A., Kai S., Sen S. Corneal keloid. Ocul Surf. 2008;6(4):186–197. - PubMed
-
- Bakhtiari P., Agarwal D.R., Fernandez A.A. Corneal keloid: report of natural history and outcome of surgical management in two cases. Cornea. 2013;32(12):1621–1624. - PubMed
-
- Fukuda K., Chikama T., Takahashi M., Nishida T. Long-term follow-up after lamellar keratoplasty in a patient with bilateral idiopathic corneal keloid. Cornea. 2011;30(12):1491–1494. - PubMed
-
- Cibis G.W., Tripathi R.C., Tripathi B.J. Corneal keloid in Lowe's syndrome. Arch Ophthalmol. 1982;100(11):1795–1799. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
