

The spectrum of biochemical alterations associated with organ dysfunction and inflammatory status and their association with disease outcomes in severe COVID-19: A longitudinal cohort and time-series design study
- PMID: 32984786
- PMCID: PMC7502281
- DOI: 10.1016/j.eclinm.2020.100554
The spectrum of biochemical alterations associated with organ dysfunction and inflammatory status and their association with disease outcomes in severe COVID-19: A longitudinal cohort and time-series design study
Abstract
Background: In patients with severe COVID-19, no data are available on the longitudinal evolution of biochemical abnormalities and their ability to predict disease outcomes.
Methods: Using a retrospective, longitudinal cohort study design on consecutive patients with severe COVID-19, we used an extensive biochemical dataset of serial data and time-series design to estimate the occurrence of organ dysfunction and the severity of the inflammatory reaction and their association with acute respiratory failure (ARF) and death.
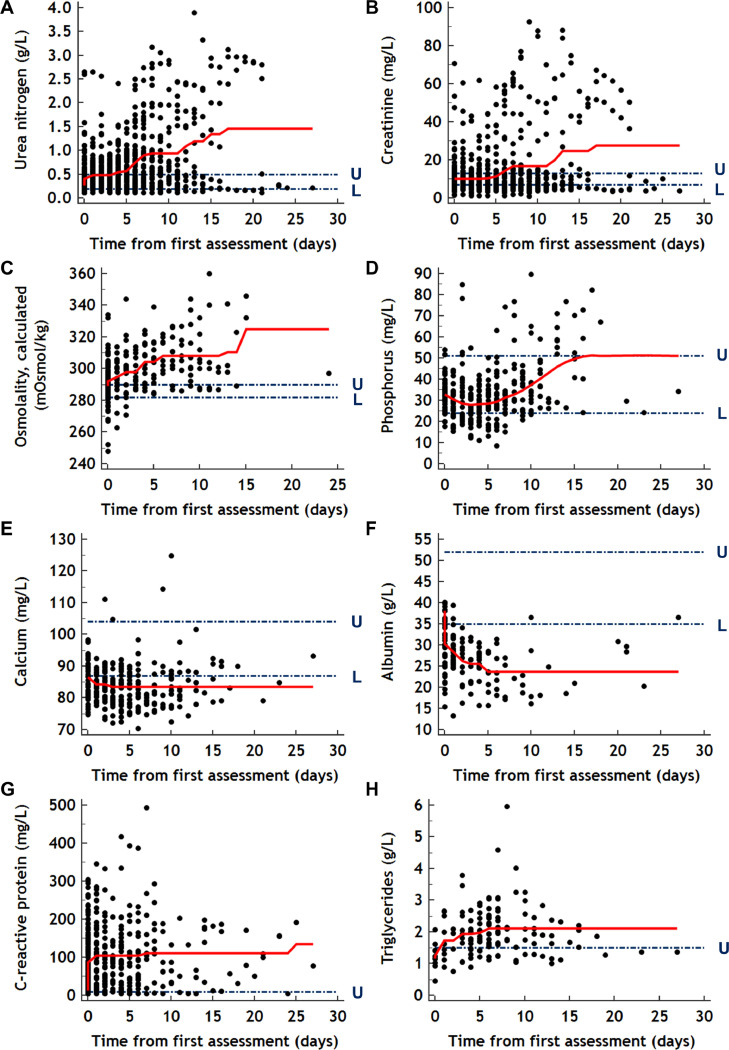
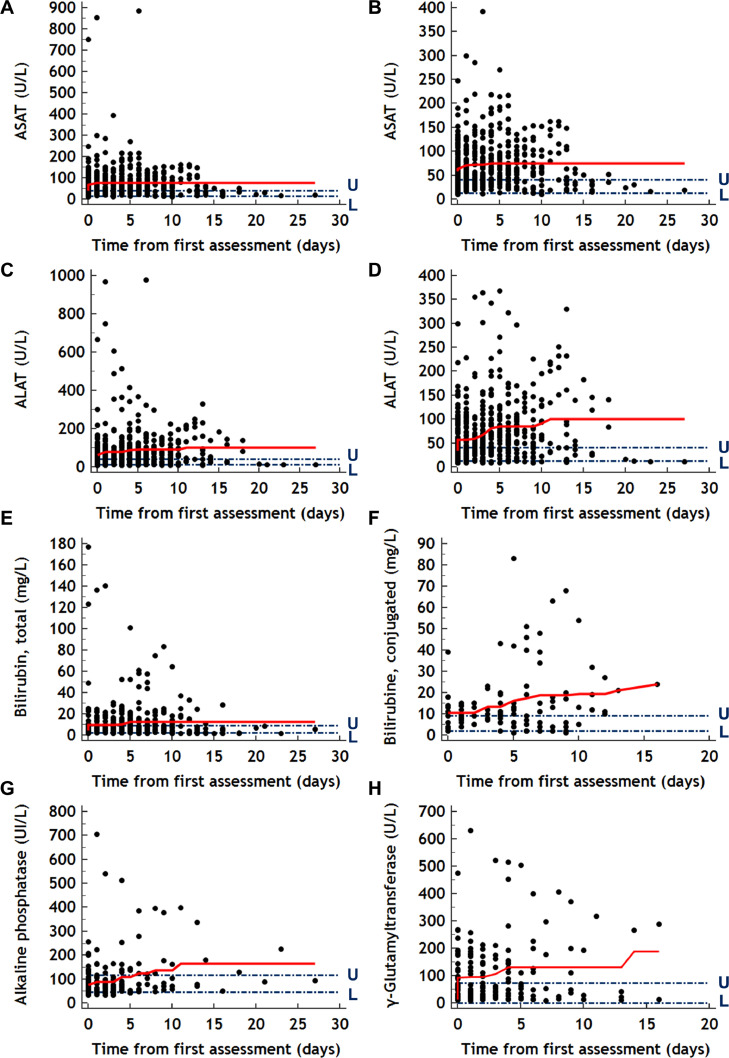
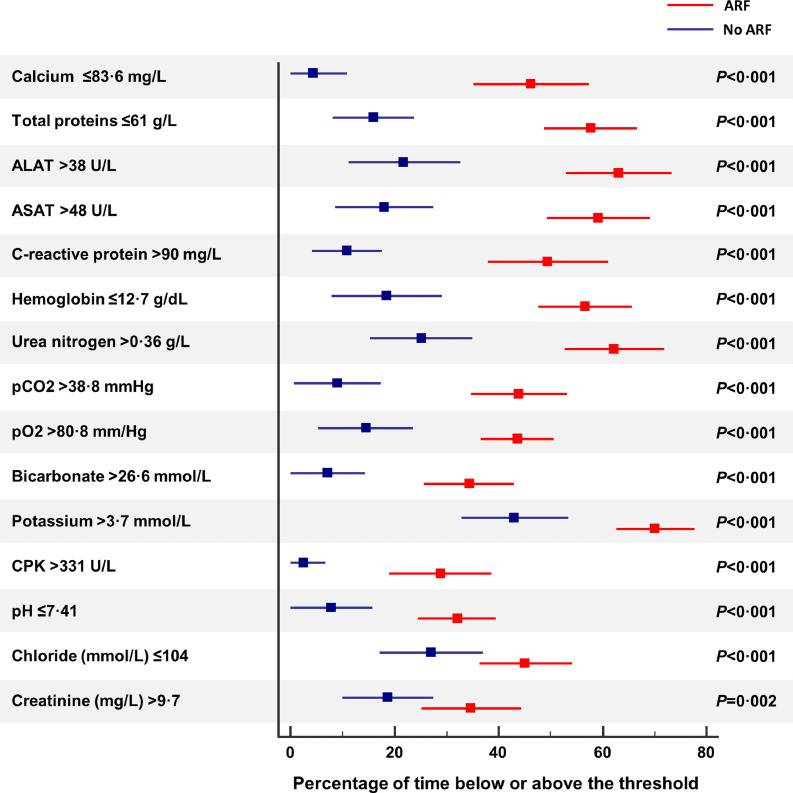
Findings: On the 162 studied patients, 1151 biochemical explorations were carried out for up to 59 biochemical markers, totaling 15,260 biochemical values. The spectrum of biochemical abnormalities and their kinetics were consistent with a multi-organ involvement, including lung, kidney, heart, liver, muscle, and pancreas, along with a severe inflammatory syndrome. The proportion of patients who developed an acute kidney injury (AKI) stage 3, increased significantly during follow-up (0·9%, day 0; 21·4%, day 14; P<0·001). On the 20 more representative biochemical markers (>250 iterations), only CRP >90 mg/L (odds ratio [OR] 6·87, 95% CI, 2·36-20·01) and urea nitrogen >0·36 g/L (OR 3·91, 95% CI, 1·15-13·29) were independently associated with the risk of ARF. Urea nitrogen >0·42 g/L was the only marker associated with the risk of COVID-19 related death.
Interpretation: Our results point out the lack of the association between the inflammatory markers and the risk of death but rather highlight a significant association between renal dysfunction and the risk of COVID-19 related acute respiratory failure and death.
© 2020 The Author(s).
Conflict of interest statement
The authors who have taken part in this study declare that they do not have anything to disclose regarding conflicts of interest concerning this manuscript.
Figures



References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
