

Therapeutic Strategy of Percutaneous Transforaminal Endoscopic Decompression for Stenosis Associated With Adult Degenerative Scoliosis
- PMID: 32985251
- PMCID: PMC9109567
- DOI: 10.1177/2192568220959036
Therapeutic Strategy of Percutaneous Transforaminal Endoscopic Decompression for Stenosis Associated With Adult Degenerative Scoliosis
Abstract
Study design: A retrospective study.
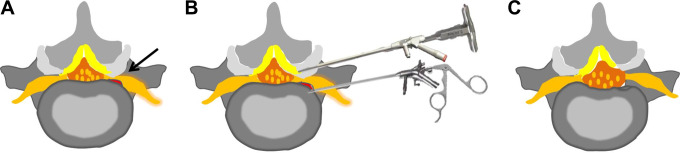
Objective: To investigate the effects of percutaneous transforaminal endoscopic decompression (PTED) for lumbar stenosis associated with adult degenerative scoliosis and to analyze the correlation between preoperative radiological parameters and postoperative surgical outcomes.
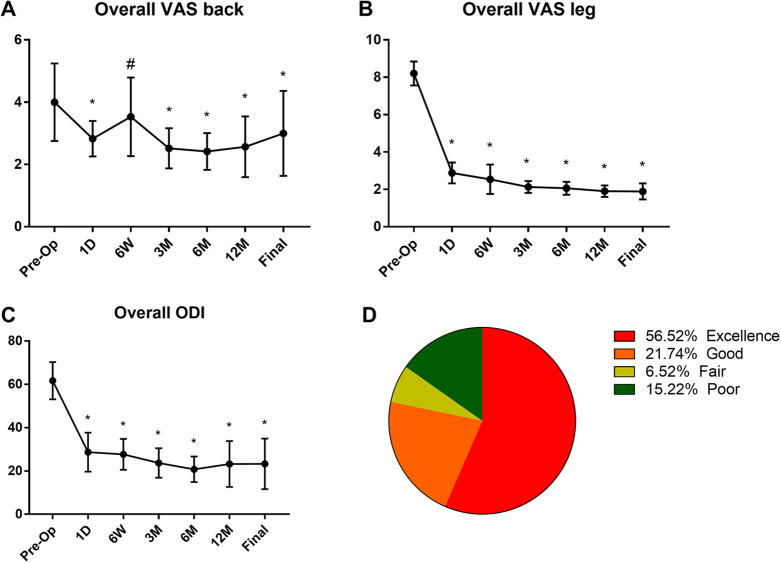
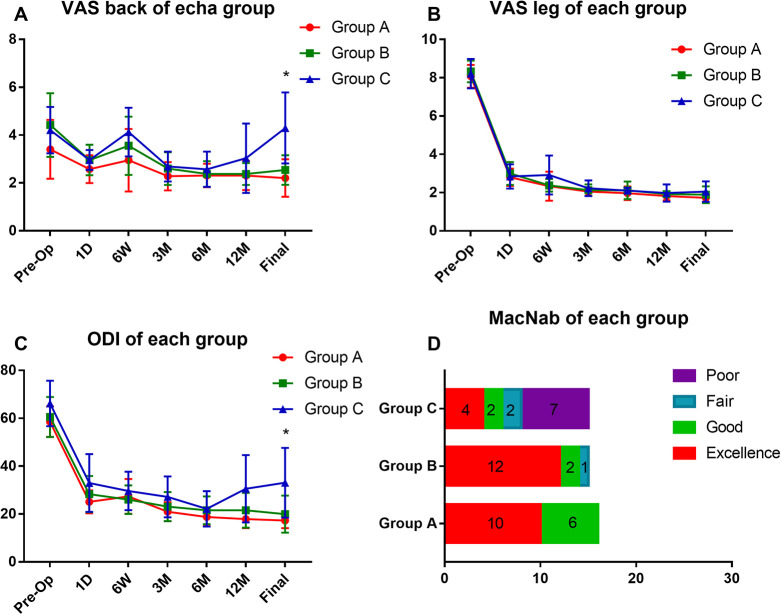
Methods: Two years of retrospective data was collected from 46 patients with lumbar stenosis associated with adult degenerative scoliosis who underwent PTED. The visual analog scale (VAS), Oswestry Disability Index, and modified MacNab criteria were used to evaluate the clinical outcomes. Multiple linear regression analysis was used to analyze the correlation between radiological parameters and surgical outcomes.
Results: The mean age of the 33 female and 13 male patients was 73.5 ± 8.1 years. The mean follow-up was 27.6 ± 3.5 months (range from 24 to 36). The average coronal Cobb angle was 24.5 ± 8.2°. There were better outcomes of the VAS for leg pain and Oswestry Disability Index after surgery. Based on the MacNab criteria, excellent or good outcomes were noted in 84.78% of patients. Multiple linear regression analysis showed that Cobb angle and lateral olisthy may be the predictors for low back pain.
Conclusion: Transforaminal endoscopic surgery may be an effective and safe method for geriatric patients with lumbar stenosis associated with degenerative scoliosis. The predictive factors of clinical outcomes were severe Cobb angle and high degree lateral subluxation. Transforaminal endoscopic surgery may not be recommended for patients with Cobb angle larger than 30° combined with lateral subluxation.
Keywords: adult degenerative scoliosis; decompression alone; percutaneous endoscopic; stenosis.
Conflict of interest statement
Figures
Similar articles
-
Comparison of percutaneous transforaminal endoscopic decompression and short-segment fusion in the treatment of elderly degenerative lumbar scoliosis with spinal stenosis.BMC Musculoskelet Disord. 2021 Oct 28;22(1):906. doi: 10.1186/s12891-021-04804-6. BMC Musculoskelet Disord. 2021. PMID: 34711184 Free PMC article.
-
Transforaminal Endoscopic Decompression Alone Versus Limited Decompression/Fusion in the Treatment of Adult Degenerative Scoliosis: A Retrospective Study.Global Spine J. 2025 May;15(4):2140-2151. doi: 10.1177/21925682241288189. Epub 2024 Sep 25. Global Spine J. 2025. PMID: 39322585 Free PMC article.
-
Transforaminal Endoscopic Discectomy and Foraminoplasty for Treating Central Lumbar Stenosis.Orthop Surg. 2019 Dec;11(6):1093-1100. doi: 10.1111/os.12559. Epub 2019 Nov 12. Orthop Surg. 2019. PMID: 31714030 Free PMC article.
-
Efficacy of percutaneous transforaminal endoscopic decompression treatment for degenerative lumbar spondylolisthesis with spinal stenosis in elderly patients.Exp Ther Med. 2020 Feb;19(2):1417-1424. doi: 10.3892/etm.2019.8337. Epub 2019 Dec 17. Exp Ther Med. 2020. PMID: 32010317 Free PMC article.
-
Technical Considerations of Uniportal Endoscopic Posterolateral Lumbar Interbody Fusion: A Review of Its Early Clinical Results in Application in Adult Degenerative Scoliosis.World Neurosurg. 2021 Jan;145:682-692. doi: 10.1016/j.wneu.2020.05.239. Epub 2020 Jun 9. World Neurosurg. 2021. PMID: 32531438 Review.
Cited by
-
Clinical outcomes of percutaneous transforaminal endoscopic decompression for the treatment of degenerative lumbar scoliosis associated with spinal stenosis in elderly individuals: a matched comparison study.Int Orthop. 2024 Dec;48(12):3197-3205. doi: 10.1007/s00264-024-06318-x. Epub 2024 Sep 25. Int Orthop. 2024. PMID: 39320498
-
Decompression Alone in the Setting of Adult Degenerative Lumbar Scoliosis and Stenosis: A Systematic Review and Meta-Analysis.Global Spine J. 2023 Apr;13(3):861-872. doi: 10.1177/21925682221127955. Epub 2022 Sep 20. Global Spine J. 2023. PMID: 36127159 Free PMC article.
-
Comparison of percutaneous transforaminal endoscopic decompression and short-segment fusion in the treatment of elderly degenerative lumbar scoliosis with spinal stenosis.BMC Musculoskelet Disord. 2021 Oct 28;22(1):906. doi: 10.1186/s12891-021-04804-6. BMC Musculoskelet Disord. 2021. PMID: 34711184 Free PMC article.
-
Characteristics of the paravertebral muscle in adult degenerative scoliosis with PI-LL match or mismatch and risk factors for PI-LL mismatch.Front Surg. 2023 Mar 29;10:1111024. doi: 10.3389/fsurg.2023.1111024. eCollection 2023. Front Surg. 2023. PMID: 37065994 Free PMC article.
-
Transforaminal Endoscopic Decompression Alone Versus Limited Decompression/Fusion in the Treatment of Adult Degenerative Scoliosis: A Retrospective Study.Global Spine J. 2025 May;15(4):2140-2151. doi: 10.1177/21925682241288189. Epub 2024 Sep 25. Global Spine J. 2025. PMID: 39322585 Free PMC article.
References
-
- Silva FE, Lenke LG. Adult degenerative scoliosis: evaluation and management. Neurosurg Focus. 2010;28:E1. - PubMed
-
- Kebaish KM, Neubauer PR, Voros GD, Khoshnevisan MA, Skolasky RL. Scoliosis in adults aged forty years and older: prevalence and relationship to age, race, and gender. Spine (Phila Pa 1976). 2011;36:731–736. - PubMed
-
- Hong JY, Suh SW, Modi HN, Hur CY, Song HR, Park JH. The prevalence and radiological findings in 1347 elderly patients with scoliosis. J Bone Joint Surg Br. 2010;92:980–983. - PubMed
-
- Koerner JD, Reitman CA, Arnold PM, Rihn J. Degenerative lumbar scoliosis. JBJS Rev. 2015;3(4). - PubMed
-
- Urrutia J, Diaz-Ledezma C, Espinosa J, Berven SH. Lumbar scoliosis in postmenopausal women: prevalence and relationship with bone density, age, and body mass index. Spine (Phila Pa 1976). 2011;36:737–740. - PubMed
LinkOut - more resources
Full Text Sources
