

Data-driven malaria prevalence prediction in large densely populated urban holoendemic sub-Saharan West Africa
- PMID: 32985514
- PMCID: PMC7522256
- DOI: 10.1038/s41598-020-72575-6
Data-driven malaria prevalence prediction in large densely populated urban holoendemic sub-Saharan West Africa
Abstract
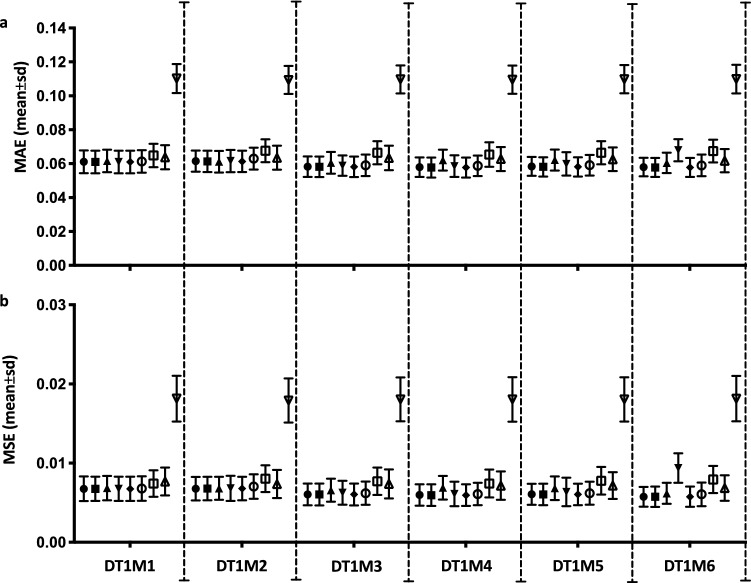
Over 200 million malaria cases globally lead to half-million deaths annually. The development of malaria prevalence prediction systems to support malaria care pathways has been hindered by lack of data, a tendency towards universal "monolithic" models (one-size-fits-all-regions) and a focus on long lead time predictions. Current systems do not provide short-term local predictions at an accuracy suitable for deployment in clinical practice. Here we show a data-driven approach that reliably produces one-month-ahead prevalence prediction within a densely populated all-year-round malaria metropolis of over 3.5 million inhabitants situated in Nigeria which has one of the largest global burdens of P. falciparum malaria. We estimate one-month-ahead prevalence in a unique 22-years prospective regional dataset of > 9 × 104 participants attending our healthcare services. Our system agrees with both magnitude and direction of the prediction on validation data achieving MAE ≤ 6 × 10-2, MSE ≤ 7 × 10-3, PCC (median 0.63, IQR 0.3) and with more than 80% of estimates within a (+ 0.1 to - 0.05) error-tolerance range which is clinically relevant for decision-support in our holoendemic setting. Our data-driven approach could facilitate healthcare systems to harness their own data to support local malaria care pathways.
Conflict of interest statement
The authors declare no competing interests.
Figures







References
-
- World Health Organization. World Malaria Report 2017. https://www.who.int/malaria/publications/world-malaria-report-2017/en/ (2017).
-
- World Health Organization. World Malaria Report 2018. https://www.who.int/malaria/publications/world-malaria-report-2018/en/ (2018).
-
- World Health Organisation. Malaria in children under five. https://www.who.int/malaria/areas/high_risk_groups/children/en/ (2018).
-
- World Health Organization. Global Technical Strategy for Malaria 2016–2030. Resolution WHA68.2. https://www.who.int/malaria/areas/global_technical_strategy/en/ (2015).
-
- World Health Organization. Overview of malaria surveillance. https://www.who.int/malaria/areas/surveillance/overview/en/ (2015).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
