

Comparison by Race of Conservative Management for Low-Risk and Intermediate-Risk Prostate Cancers in Veterans From 2004 to 2018
- PMID: 32986109
- PMCID: PMC7522702
- DOI: 10.1001/jamanetworkopen.2020.18318
Comparison by Race of Conservative Management for Low-Risk and Intermediate-Risk Prostate Cancers in Veterans From 2004 to 2018
Abstract
Importance: Conservative management (ie, active surveillance or watchful waiting) is a guideline-based strategy for men with low-risk and intermediate-risk prostate cancer. However, use of conservative management is controversial for African American patients, who have worse prostate cancer outcomes compared with White patients.
Objective: To examine the association of African American race with the receipt and duration of conservative management in the Veterans Health Administration (VA), a large equal-access health system.
Design, setting, and participants: This cohort study used data from the VA Corporate Data Warehouse for 51 543 African American and non-Hispanic White veterans diagnosed with low-risk and intermediate-risk localized node-negative prostate cancer between January 1, 2004, and December 31, 2013. Men who did not receive continuous VA care were excluded. Data were analyzed from February 1 to June 30, 2020.
Exposures: All patients received either definitive therapy (ie, prostatectomy, radiation, androgen deprivation therapy) or conservative management (ie, active surveillance or watchful waiting).
Main outcomes and measures: Receipt of conservative management and (for patients receiving conservative management) time from diagnosis to definitive therapy.
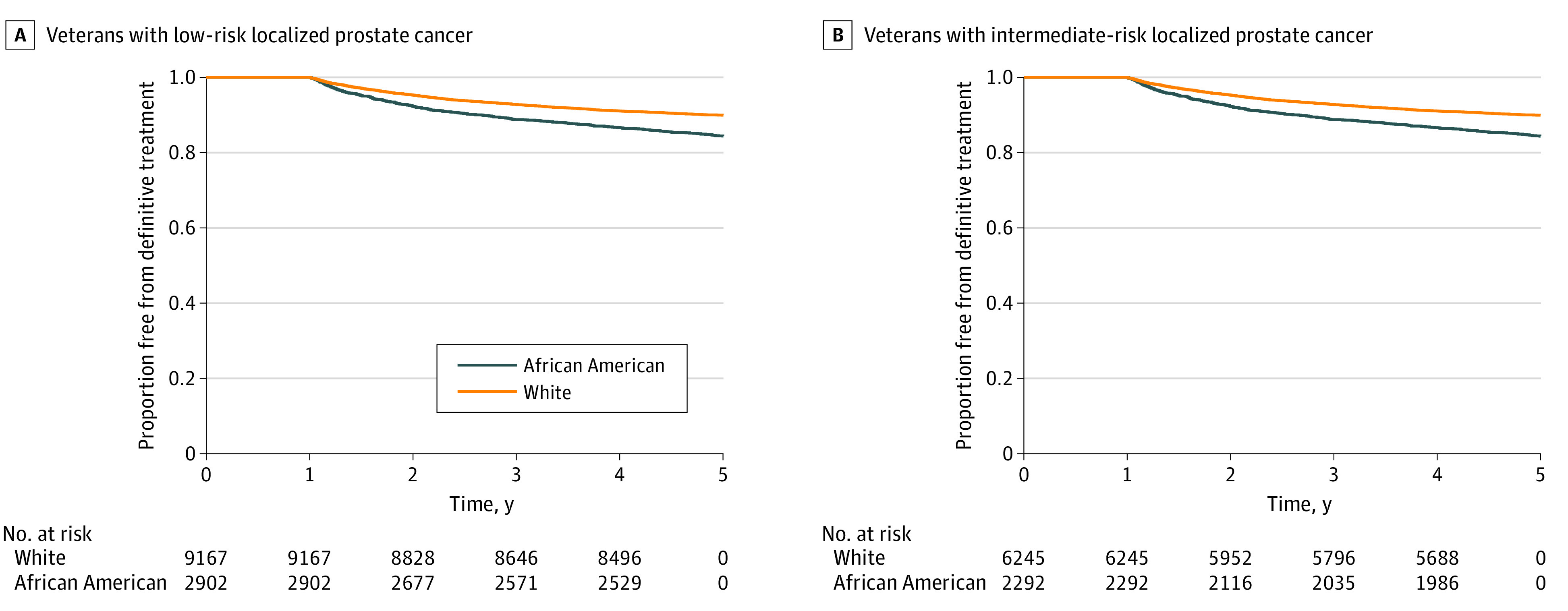
Results: The median (interquartile range) age of the 51 543 veterans in our cohort was 65 (61-70) years, and 14 830 veterans (28.8%) were African American individuals. Compared with White veterans, African American veterans were more likely to have intermediate-risk disease (18 988 [51.7%] vs 8526 [57.5%]), 3 or more comorbidities (15 438 [42.1%] vs 7614 [51.3%]), and high disability-related or income-related needs (9078 [24.7%] vs 4614 [31.1%]). Overall, 20 606 veterans (40.0%) received conservative management. African American veterans with low-risk disease (adjusted relative risk, 0.95; 95% CI, 0.92-0.98; P < .001) and intermediate-risk disease (adjusted relative risk, 0.92; 95% CI, 0.87-0.97; P = .002) were less likely to receive conservative management than White veterans. Compared with White veterans, African American veterans with low-risk disease (adjusted hazard ratio, 1.71; 95% CI, 1.50-1.95; P < .001) and intermediate-risk disease (adjusted hazard ratio, 1.46; 95% CI, 1.27-1.69; P < .001) who received conservative management were more likely to receive definitive therapy within 5 years of diagnosis (restricted mean survival time [SE] at 5 years, 1679 [5.3] days vs 1740 [2.4] days; P < .001).
Conclusions and relevance: In this study, conservative management was less commonly used and less durable for African American veterans than for White veterans. Prospective trials should assess the comparative effectiveness of conservative management in African American men with prostate cancer.
Conflict of interest statement
Figures

References
-
- Mohler JL, Horwitz EM, Richey S. NCCN Guidelines Index table of contents discussion. Prostate Cancer. 2020;167:479-505.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
