

Long-term survival of children born with congenital anomalies: A systematic review and meta-analysis of population-based studies
- PMID: 32986711
- PMCID: PMC7521740
- DOI: 10.1371/journal.pmed.1003356
Long-term survival of children born with congenital anomalies: A systematic review and meta-analysis of population-based studies
Abstract
Background: Following a reduction in global child mortality due to communicable diseases, the relative contribution of congenital anomalies to child mortality is increasing. Although infant survival of children born with congenital anomalies has improved for many anomaly types in recent decades, there is less evidence on survival beyond infancy. We aimed to systematically review, summarise, and quantify the existing population-based data on long-term survival of individuals born with specific major congenital anomalies and examine the factors associated with survival.
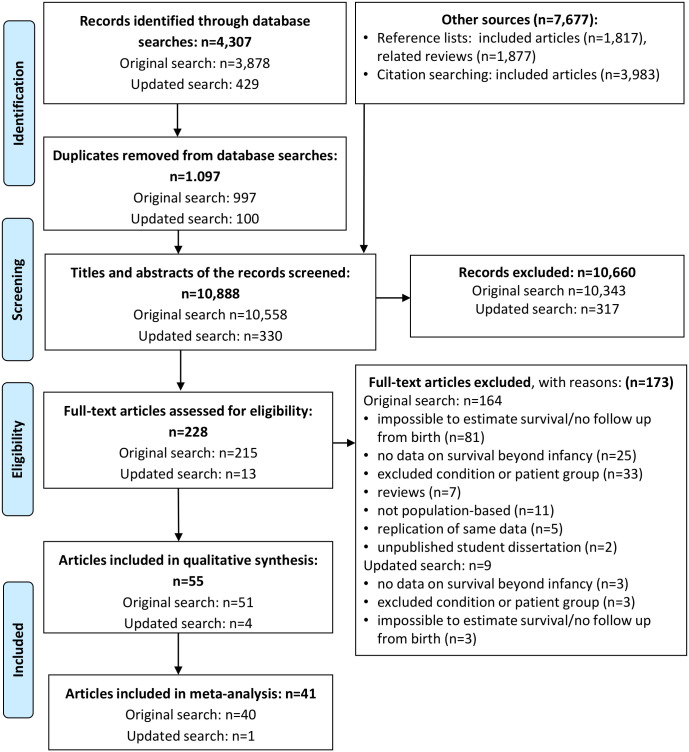
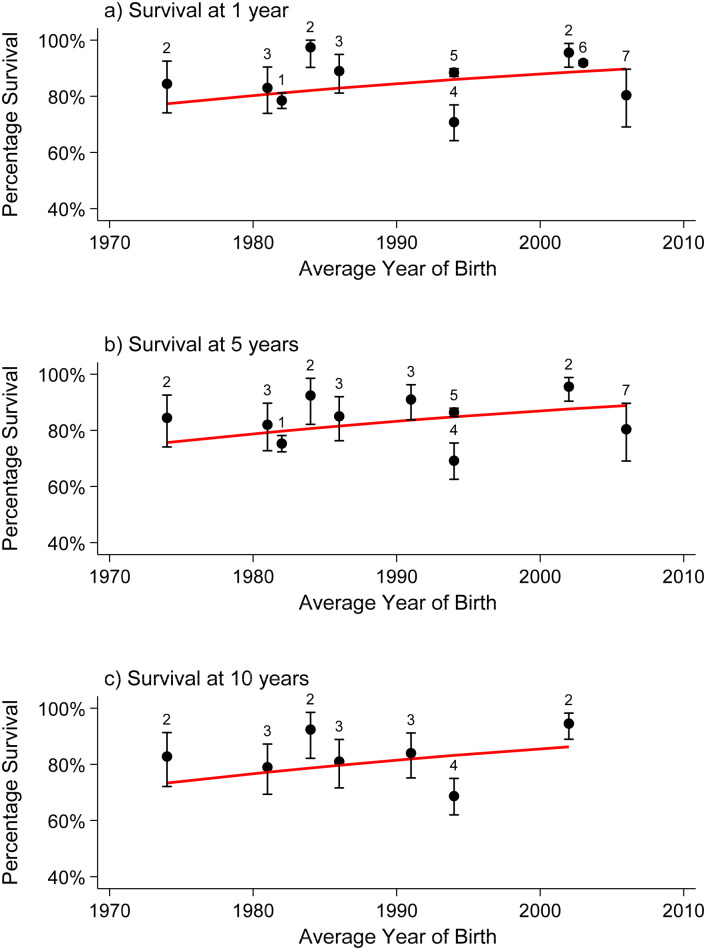
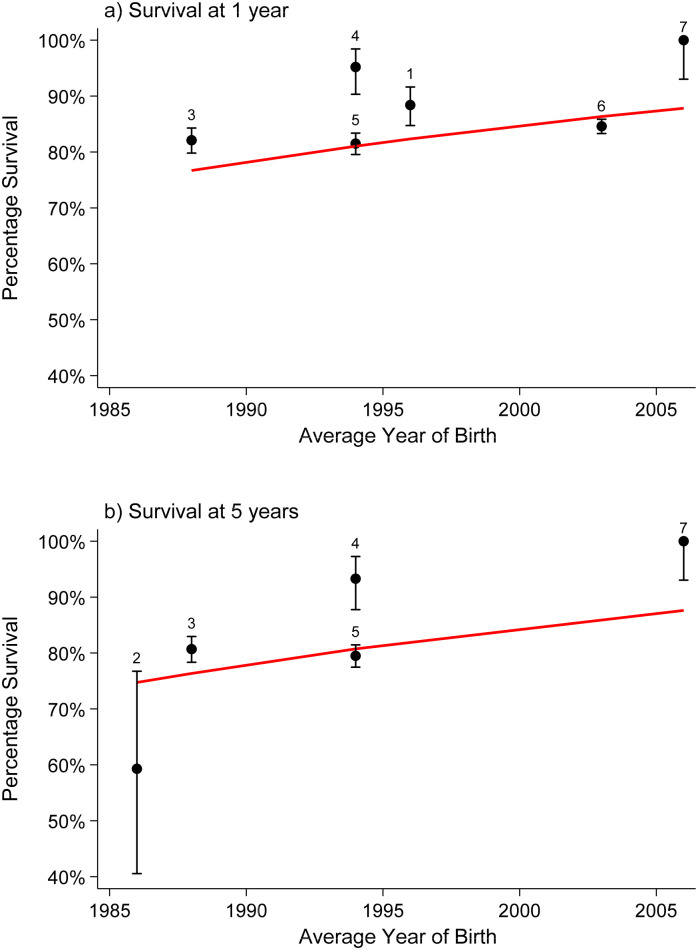
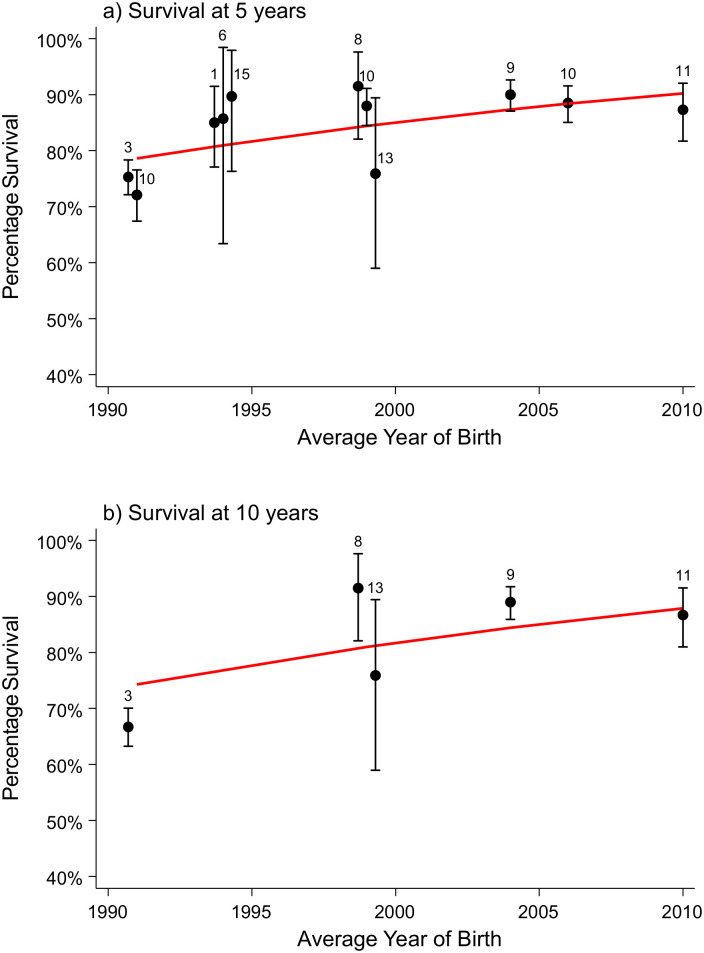
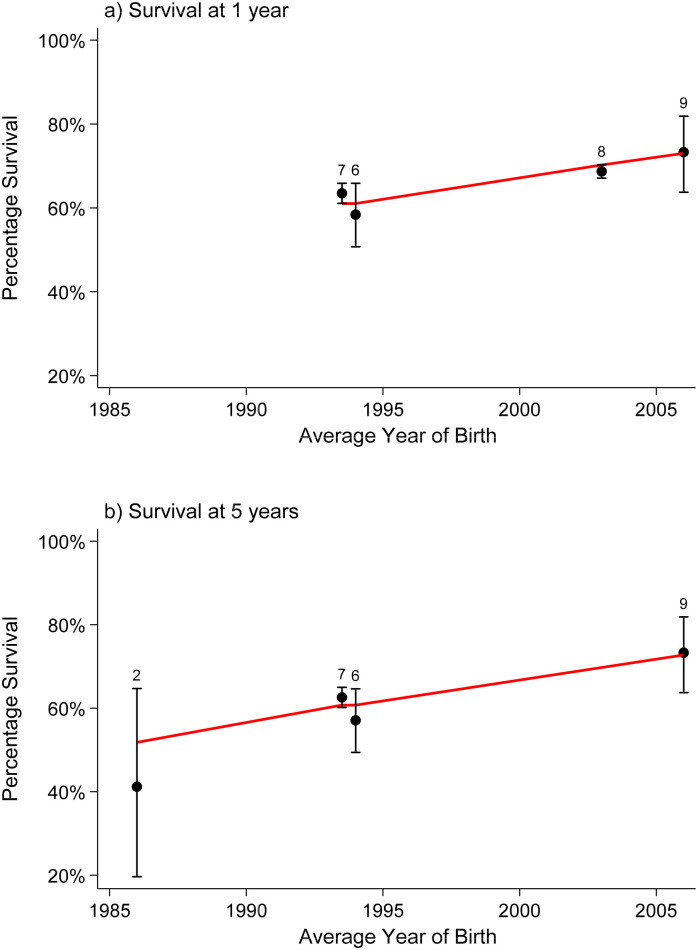
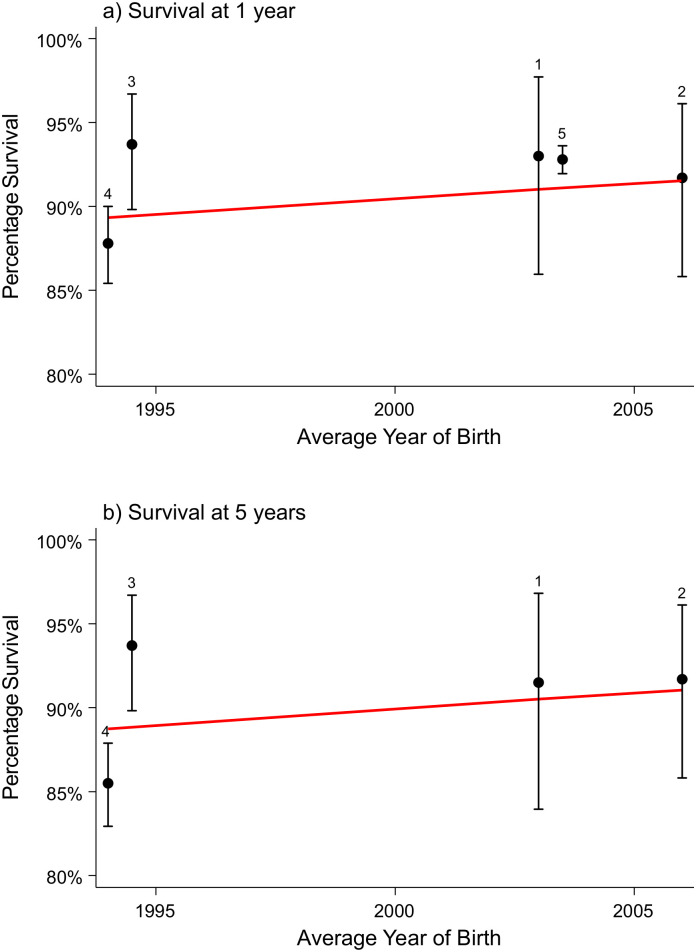
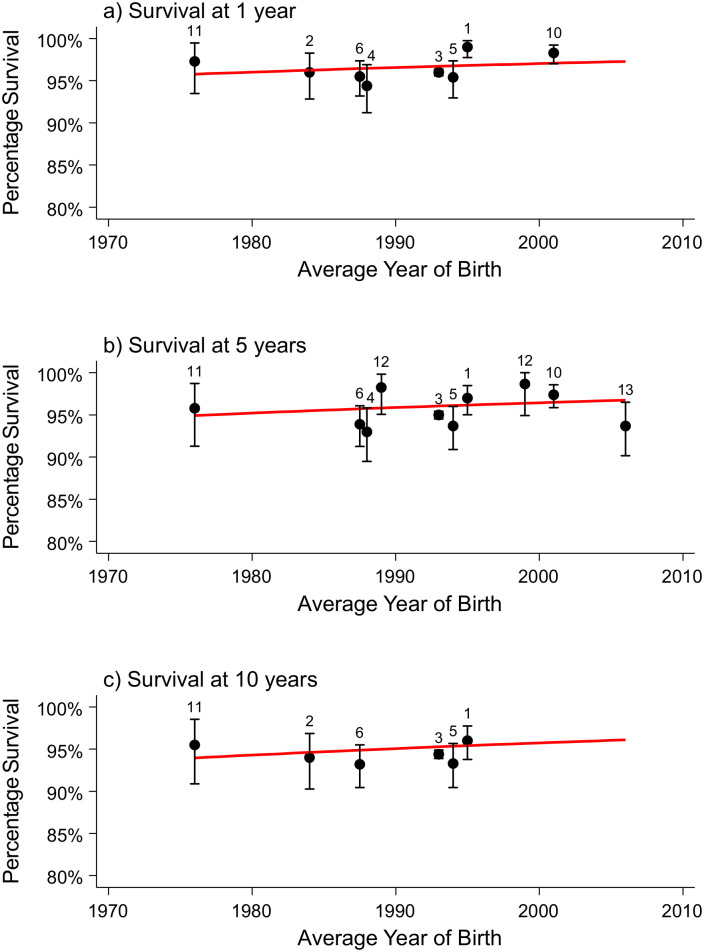
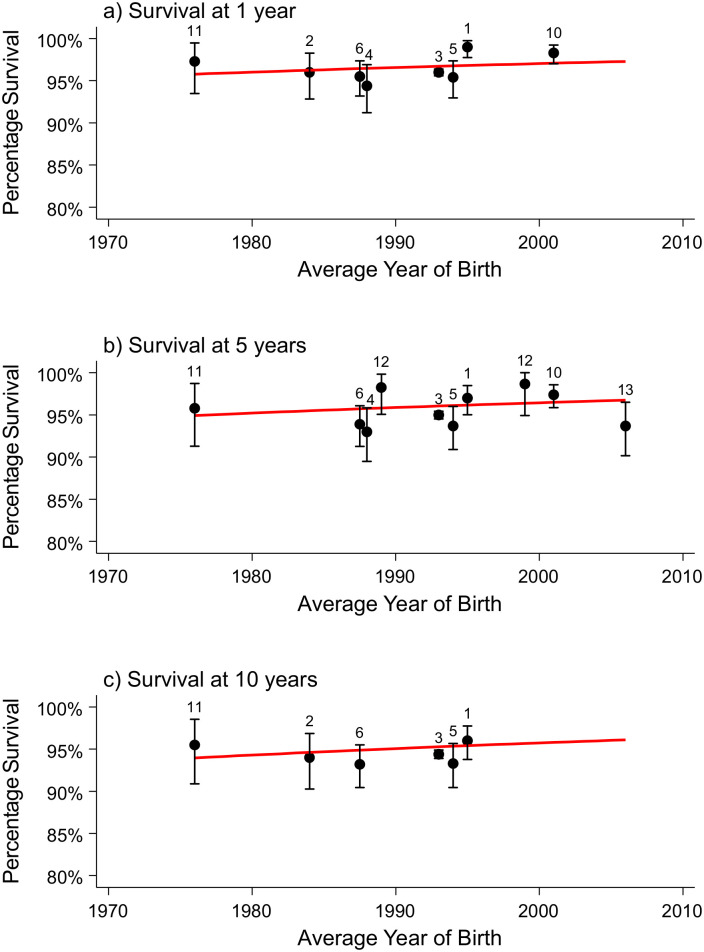
Methods and findings: Seven electronic databases (Medline, Embase, Scopus, PsycINFO, CINAHL, ProQuest Natural, and Biological Science Collections), reference lists, and citations of the included articles for studies published 1 January 1995 to 30 April 2020 were searched. Screening for eligibility, data extraction, and quality appraisal were performed in duplicate. We included original population-based studies that reported long-term survival (beyond 1 year of life) of children born with a major congenital anomaly with the follow-up starting from birth that were published in the English language as peer-reviewed papers. Studies on congenital heart defects (CHDs) were excluded because of a recent systematic review of population-based studies of CHD survival. Meta-analysis was performed to pool survival estimates, accounting for trends over time. Of 10,888 identified articles, 55 (n = 367,801 live births) met the inclusion criteria and were summarised narratively, 41 studies (n = 54,676) investigating eight congenital anomaly types (spina bifida [n = 7,422], encephalocele [n = 1,562], oesophageal atresia [n = 6,303], biliary atresia [n = 3,877], diaphragmatic hernia [n = 6,176], gastroschisis [n = 4,845], Down syndrome by presence of CHD [n = 22,317], and trisomy 18 [n = 2,174]) were included in the meta-analysis. These studies covered birth years from 1970 to 2015. Survival for children with spina bifida, oesophageal atresia, biliary atresia, diaphragmatic hernia, gastroschisis, and Down syndrome with an associated CHD has significantly improved over time, with the pooled odds ratios (ORs) of surviving per 10-year increase in birth year being OR = 1.34 (95% confidence interval [95% CI] 1.24-1.46), OR = 1.50 (95% CI 1.38-1.62), OR = 1.62 (95% CI 1.28-2.05), OR = 1.57 (95% CI 1.37-1.81), OR = 1.24 (95% CI 1.02-1.5), and OR = 1.99 (95% CI 1.67-2.37), respectively (p < 0.001 for all, except for gastroschisis [p = 0.029]). There was no observed improvement for children with encephalocele (OR = 0.98, 95% CI 0.95-1.01, p = 0.19) and children with biliary atresia surviving with native liver (OR = 0.96, 95% CI 0.88-1.03, p = 0.26). The presence of additional structural anomalies, low birth weight, and earlier year of birth were the most commonly reported predictors of reduced survival for any congenital anomaly type. The main limitation of the meta-analysis was the small number of studies and the small size of the cohorts, which limited the predictive capabilities of the models resulting in wide confidence intervals.
Conclusions: This systematic review and meta-analysis summarises estimates of long-term survival associated with major congenital anomalies. We report a significant improvement in survival of children with specific congenital anomalies over the last few decades and predict survival estimates up to 20 years of age for those born in 2020. This information is important for the planning and delivery of specialised medical, social, and education services and for counselling affected families. This trial was registered on the PROSPERO database (CRD42017074675).
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Socio-economic inequalities in mortality in children with congenital heart disease: A systematic review and meta-analysis.Paediatr Perinat Epidemiol. 2019 Jul;33(4):291-309. doi: 10.1111/ppe.12564. Paediatr Perinat Epidemiol. 2019. PMID: 31347722
-
Major Congenital Anomalies in Korean Livebirths in 2013-2014: Based on the National Health Insurance Database.J Korean Med Sci. 2023 Oct 9;38(39):e304. doi: 10.3346/jkms.2023.38.e304. J Korean Med Sci. 2023. PMID: 37821084 Free PMC article.
-
Ten-Year Survival of Children With Congenital Anomalies: A European Cohort Study.Pediatrics. 2022 Mar 1;149(3):e2021053793. doi: 10.1542/peds.2021-053793. Pediatrics. 2022. PMID: 35146505
-
The Association of Prenatal Diagnoses with Mortality and Long-Term Morbidity in Children with Specific Isolated Congenital Anomalies: A European Register-Based Cohort Study.Matern Child Health J. 2024 Jun;28(6):1020-1030. doi: 10.1007/s10995-024-03911-9. Epub 2024 Mar 4. Matern Child Health J. 2024. PMID: 38438690 Free PMC article.
-
Environmental and individual exposure and the risk of congenital anomalies: a review of recent epidemiological evidence.Epidemiol Prev. 2018 May-Aug;42(3-4 Suppl 1):1-34. doi: 10.19191/EP18.3-4.S1.P001.057. Epidemiol Prev. 2018. PMID: 30066535 Review. English.
Cited by
-
Ambient air pollutants in the first trimester of pregnancy and birth defects: an observational study.BMJ Open. 2023 Mar 22;13(3):e063712. doi: 10.1136/bmjopen-2022-063712. BMJ Open. 2023. PMID: 36948563 Free PMC article.
-
Hospital length of stay among children with and without congenital anomalies across 11 European regions-A population-based data linkage study.PLoS One. 2022 Jul 22;17(7):e0269874. doi: 10.1371/journal.pone.0269874. eCollection 2022. PLoS One. 2022. PMID: 35867669 Free PMC article.
-
Mothers of children with major congenital anomalies have increased health care utilization over a 20-year post-birth time horizon.PLoS One. 2021 Dec 8;16(12):e0260962. doi: 10.1371/journal.pone.0260962. eCollection 2021. PLoS One. 2021. PMID: 34879106 Free PMC article.
-
Psychosocial needs and outcomes of adults with spina bifida: A scoping review, 1974-2023.Health Care Transit. 2024 Feb 14;2:100041. doi: 10.1016/j.hctj.2024.100041. eCollection 2024. Health Care Transit. 2024. PMID: 39712619 Free PMC article.
-
Beliefs and perceptions towards congenital anomalies in Dilla town, Gedeo Zone, Southern Ethiopia; a qualitative study.BMC Pediatr. 2025 Jan 11;25(1):23. doi: 10.1186/s12887-024-05257-1. BMC Pediatr. 2025. PMID: 39799322 Free PMC article.
References
-
- World Health Organization. Health 2015: from MDGs, Millennium Development Goals to SDGs, Sustainable Development Goals. Chapter 4. Snapshot: Child Health. Switzerland: WHO; 2015 [cited 2019 Dec 9]. https://www.who.int/gho/publications/mdgs-sdgs/MDGs-SDGs2015_chapter4_sn....
-
- Australian Institute of Health and Welfare. Australian children. Canberra: AIHW; 2020 [cited 2019 Dec 9]. Contract No.: Cat. no. CWS 69. https://www.aihw.gov.au/getmedia/6af928d6-692e-4449-b915-cf2ca946982f/ai....
-
- Heron M. Deaths: Leading Causes for 2016. Natl Vital Stat Rep. 2018;67(6):1–77. . - PubMed
-
- Office for National Statistics. Child and infant mortality in England and Wales: 2016. Statistical bulletin [Internet]. 2018 [cited 2019 Dec 9]. https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarri....
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
