

Extracorporeal membrane oxygenation support in COVID-19: an international cohort study of the Extracorporeal Life Support Organization registry
- PMID: 32987008
- PMCID: PMC7518880
- DOI: 10.1016/S0140-6736(20)32008-0
Extracorporeal membrane oxygenation support in COVID-19: an international cohort study of the Extracorporeal Life Support Organization registry
Erratum in
-
Department of Error.Lancet. 2020 Oct 10;396(10257):1070. doi: 10.1016/S0140-6736(20)32082-1. Lancet. 2020. PMID: 33038966 Free PMC article. No abstract available.
Abstract
Background: Multiple major health organisations recommend the use of extracorporeal membrane oxygenation (ECMO) support for COVID-19-related acute hypoxaemic respiratory failure. However, initial reports of ECMO use in patients with COVID-19 described very high mortality and there have been no large, international cohort studies of ECMO for COVID-19 reported to date.
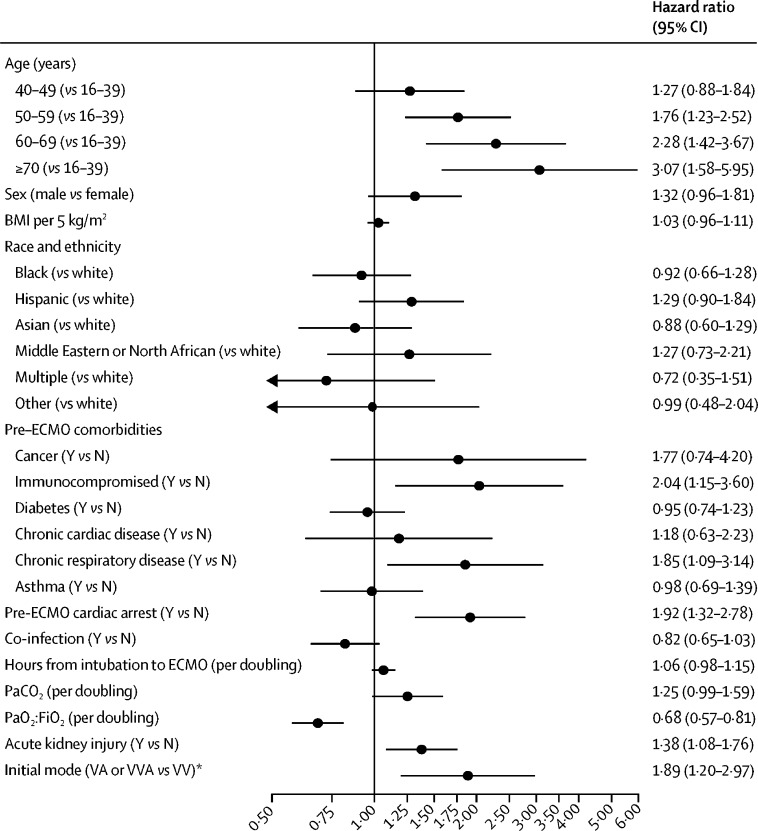
Methods: We used data from the Extracorporeal Life Support Organization (ELSO) Registry to characterise the epidemiology, hospital course, and outcomes of patients aged 16 years or older with confirmed COVID-19 who had ECMO support initiated between Jan 16 and May 1, 2020, at 213 hospitals in 36 countries. The primary outcome was in-hospital death in a time-to-event analysis assessed at 90 days after ECMO initiation. We applied a multivariable Cox model to examine whether patient and hospital factors were associated with in-hospital mortality.
Findings: Data for 1035 patients with COVID-19 who received ECMO support were included in this study. Of these, 67 (6%) remained hospitalised, 311 (30%) were discharged home or to an acute rehabilitation centre, 101 (10%) were discharged to a long-term acute care centre or unspecified location, 176 (17%) were discharged to another hospital, and 380 (37%) died. The estimated cumulative incidence of in-hospital mortality 90 days after the initiation of ECMO was 37·4% (95% CI 34·4-40·4). Mortality was 39% (380 of 968) in patients with a final disposition of death or hospital discharge. The use of ECMO for circulatory support was independently associated with higher in-hospital mortality (hazard ratio 1·89, 95% CI 1·20-2·97). In the subset of patients with COVID-19 receiving respiratory (venovenous) ECMO and characterised as having acute respiratory distress syndrome, the estimated cumulative incidence of in-hospital mortality 90 days after the initiation of ECMO was 38·0% (95% CI 34·6-41·5).
Interpretation: In patients with COVID-19 who received ECMO, both estimated mortality 90 days after ECMO and mortality in those with a final disposition of death or discharge were less than 40%. These data from 213 hospitals worldwide provide a generalisable estimate of ECMO mortality in the setting of COVID-19.
Funding: None.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Figures


Comment in
-
ECMO support for COVID-19: a balancing act.Lancet. 2021 Jan 9;397(10269):94-95. doi: 10.1016/S0140-6736(20)32515-0. Lancet. 2021. PMID: 33422255 Free PMC article. No abstract available.
-
ECMO support for COVID-19: a balancing act - Authors' reply.Lancet. 2021 Jan 9;397(10269):95. doi: 10.1016/S0140-6736(20)32517-4. Lancet. 2021. PMID: 33422256 Free PMC article. No abstract available.
-
[Focus ventilation, oxygen therapy and weaning : Intensive medical care studies from 2020/2021].Anaesthesist. 2021 Nov;70(11):967-976. doi: 10.1007/s00101-021-00979-8. Epub 2021 Oct 6. Anaesthesist. 2021. PMID: 34613457 Free PMC article. German. No abstract available.
References
-
- Combes A, Hajage D, Capellier G. Extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. N Engl J Med. 2018;378:1965–1975. - PubMed
-
- Goligher EC, Tomlinson G, Hajage D. Extracorporeal membrane oxygenation for severe acute respiratory distress syndrome and posterior probability of mortality benefit in a post hoc Bayesian analysis of a randomized clinical trial. JAMA. 2018;320:2251–2259. - PubMed
-
- Munshi L, Walkey A, Goligher E, Pham T, Uleryk EM, Fan E. Venovenous extracorporeal membrane oxygenation for acute respiratory distress syndrome: a systematic review and meta-analysis. Lancet Respir Med. 2019;7:163–172. - PubMed
