

Longitudinal anatomic, functional, and molecular characterization of Pick disease phenotypes
- PMID: 32989107
- PMCID: PMC7836669
- DOI: 10.1212/WNL.0000000000010948
Longitudinal anatomic, functional, and molecular characterization of Pick disease phenotypes
Abstract
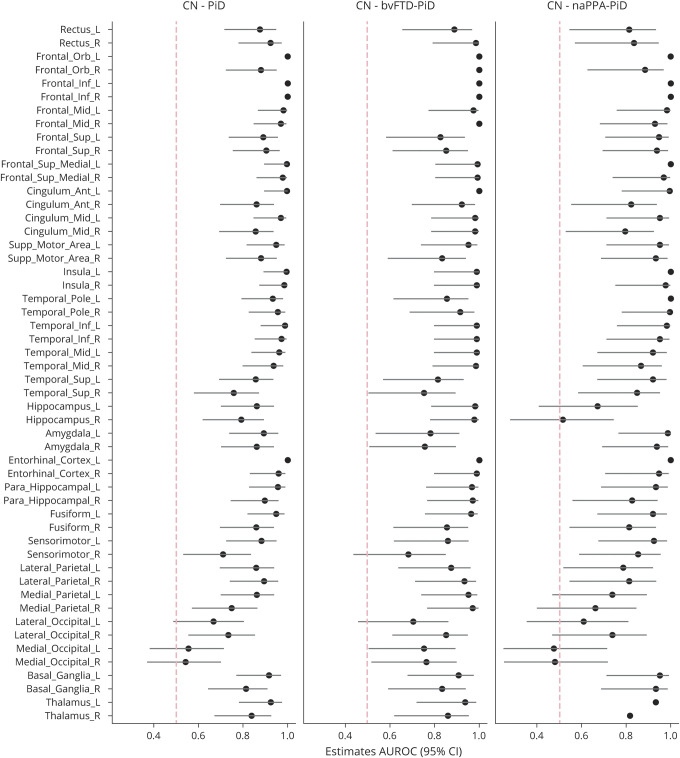
Objective: To characterize longitudinal MRI and PET abnormalities in autopsy-confirmed Pick disease (PiD) and determine how patterns of neurodegeneration differ with respect to clinical syndrome.
Methods: Seventeen patients with PiD were identified who had antemortem MRI (8 with behavioral variant frontotemporal dementia [bvFTD-PiD], 6 with nonfluent/agrammatic primary progressive aphasia [naPPA-PiD], 1 with semantic primary progressive aphasia, 1 with unclassified primary progressive aphasia, and 1 with corticobasal syndrome). Thirteen patients had serial MRI for a total of 56 MRIs, 7 had [18F]fluorodeoxyglucose PET, 4 had Pittsburgh compound B (PiB) PET, and 1 patient had [18F]flortaucipir PET. Cross-sectional and longitudinal comparisons of gray matter volume and metabolism were performed between bvFTD-PiD, naPPA-PiD, and controls. Cortical PiB summaries were calculated to determine β-amyloid positivity.
Results: The bvFTD-PiD and naPPA-PiD groups showed different foci of volume loss and hypometabolism early in the disease, with bvFTD-PiD involving bilateral prefrontal and anterior temporal cortices and naPPA-PiD involving left inferior frontal gyrus, insula, and orbitofrontal cortex. However, patterns merged over time, with progressive spread into prefrontal and anterior temporal lobe in naPPA-PiD, and eventual involvement of posterior temporal lobe, motor cortex, and parietal lobe in both groups. Rates of frontotemporal atrophy were faster in bvFTD-PiD than naPPA-PiD. One patient was β-amyloid-positive on PET with low Alzheimer neuropathologic changes at autopsy. Flortaucipir PET showed elevated uptake in frontotemporal white matter.
Conclusion: Patterns of atrophy and hypometabolism differ in PiD according to presenting syndrome, although patterns of neurodegeneration appear to converge over time.
© 2020 American Academy of Neurology.
Figures





References
-
- Dickson DW. Neuropathology of Pick's disease. Neurology 2001;56:S16–S20. - PubMed
-
- Kertesz A, McMonagle P, Blair M, Davidson W, Munoz DG. The evolution and pathology of frontotemporal dementia. Brain 2005;128:1996–2005. - PubMed
-
- Piguet O, Halliday GM, Reid WG, et al. Clinical phenotypes in autopsy-confirmed Pick disease. Neurology 2011;76:253–259. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources