Generating sequential electronic health records using dual adversarial autoencoder
- PMID: 32989459
- PMCID: PMC7647348
- DOI: 10.1093/jamia/ocaa119
Generating sequential electronic health records using dual adversarial autoencoder
Abstract
Objective: Recent studies on electronic health records (EHRs) started to learn deep generative models and synthesize a huge amount of realistic records, in order to address significant privacy issues surrounding the EHR. However, most of them only focus on structured records about patients' independent visits, rather than on chronological clinical records. In this article, we aim to learn and synthesize realistic sequences of EHRs based on the generative autoencoder.
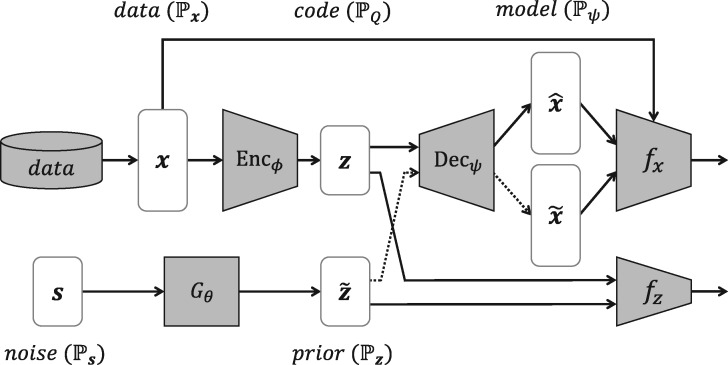
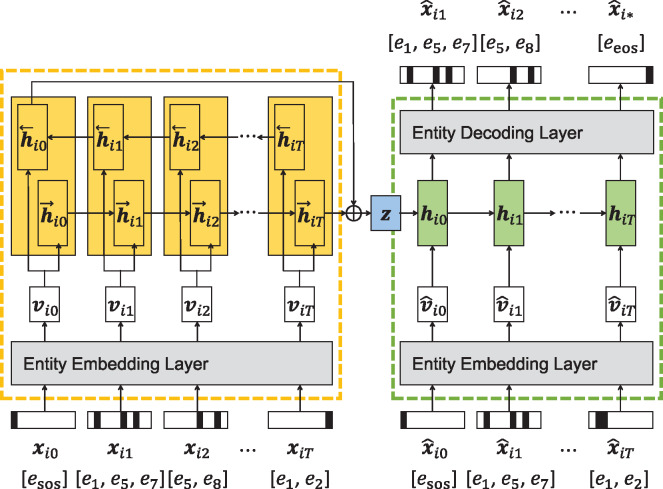
Materials and methods: We propose a dual adversarial autoencoder (DAAE), which learns set-valued sequences of medical entities, by combining a recurrent autoencoder with 2 generative adversarial networks (GANs). DAAE improves the mode coverage and quality of generated sequences by adversarially learning both the continuous latent distribution and the discrete data distribution. Using the MIMIC-III (Medical Information Mart for Intensive Care-III) and UT Physicians clinical databases, we evaluated the performances of DAAE in terms of predictive modeling, plausibility, and privacy preservation.
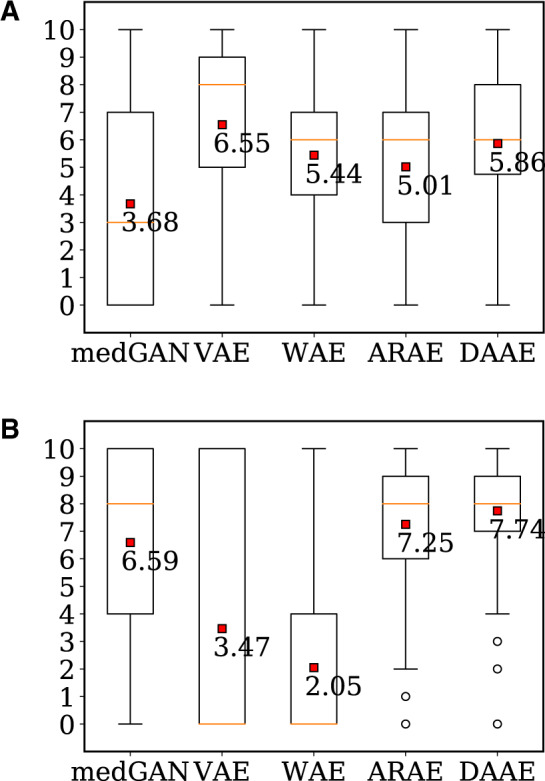
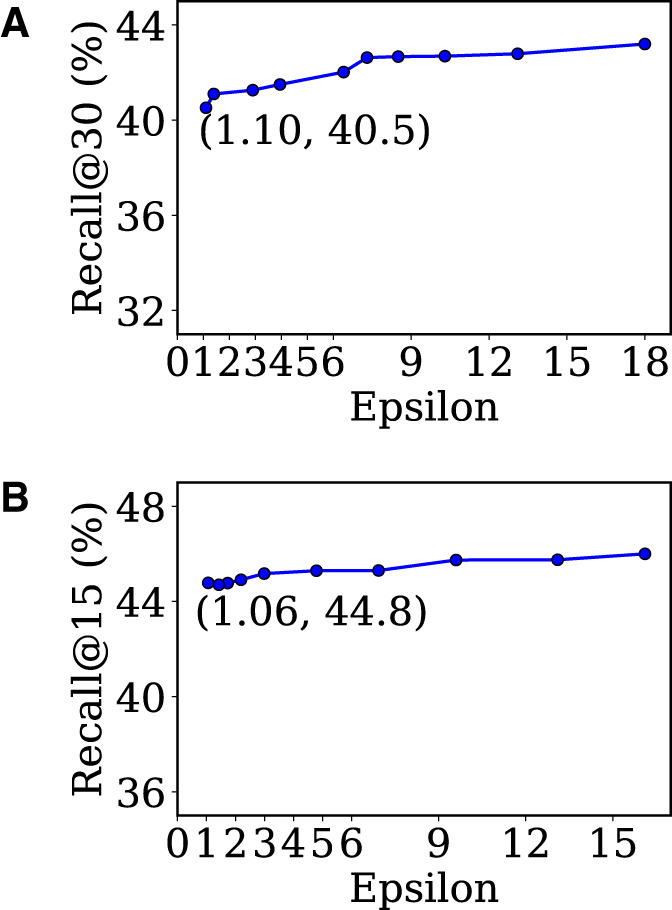
Results: Our generated sequences of EHRs showed the comparable performances to real data for a predictive modeling task, and achieved the best score in plausibility evaluation conducted by medical experts among all baseline models. In addition, differentially private optimization of our model enables to generate synthetic sequences without increasing the privacy leakage of patients' data.
Conclusions: DAAE can effectively synthesize sequential EHRs by addressing its main challenges: the synthetic records should be realistic enough not to be distinguished from the real records, and they should cover all the training patients to reproduce the performance of specific downstream tasks.
Keywords: differential privacy; electornic health records (EHRs); generative adversarial networks (GANs); generative autoencoder; sequential data generation.
© The Author(s) 2020. Published by Oxford University Press on behalf of the American Medical Informatics Association. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures