

Surgical resection does not avoid the risk of diverticulitis recurrence-a systematic review of risk factors
- PMID: 32989503
- PMCID: PMC7801345
- DOI: 10.1007/s00384-020-03762-0
Surgical resection does not avoid the risk of diverticulitis recurrence-a systematic review of risk factors
Abstract
Purpose: Fifteen percent of patients undergoing elective sigmoidectomy will present a diverticulitis recurrence, which is associated with significant costs and morbidity. We aimed to systematically review the risk factors associated with recurrence after elective sigmoidectomy.
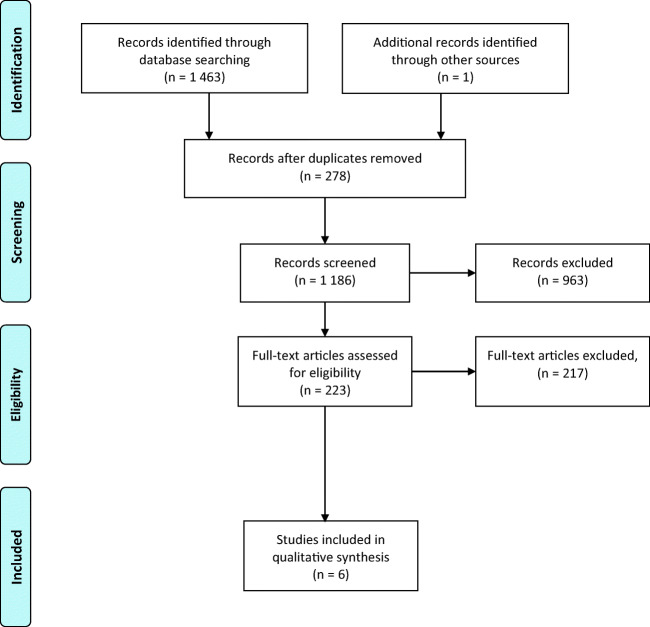
Methods: PubMed/MEDLINE, Embase, Cochrane, and Web of Science were searched for studies published until May 1, 2020. Original studies were included if (i) they included patients undergoing sigmoidectomy for diverticular disease, (ii) they reported postoperative recurrent diverticulitis, and (iii) they analyzed ≥ 1 variable associated with recurrence. The primary outcome was the risk factors for recurrence of diverticulitis after sigmoidectomy.
Results: From the 1463 studies initially screened, six studies were included. From the 1062 patients included, 62 patients recurred (5.8%), and six variables were associated with recurrence. Two were preoperative: age (HR = 0.96, p = 0.02) and irritable bowel syndrome (33.3% with recurrence versus 12.1% without recurrence, p = 0.02). Two were operative factors: uncomplicated recurrent diverticulitis as indication for surgery (73.3% with recurrence versus 49.9% without recurrence, p = 0.049) and anastomotic level (colorectal: HR = 11.4, p = 0.02, or colosigmoid: OR = 4, p = 0.033). Two were postoperative variables: the absence of active diverticulitis on pathology (39.6% with recurrence versus 26.6% without recurrence) and persistence of postoperative pain (HR = 4.8, p < 0.01).
Conclusion: Identification of preoperative variables that predict the occurrence of diverticulitis recurrence should help surgical decision-making for elective sigmoidectomy, while peri- and postoperative factors should be taken into account for optimal patient follow-up.
Keywords: Diverticulitis; Postoperative recurrence; Risk factors; Sigmoidectomy.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Jacobs DO. Clinical practice. Diverticulitis. N Engl J Med. 2007;357(20):2057–2066. - PubMed
-
- Wasvary H, Turfah F, Kadro O, Beauregard W. Same hospitalization resection for acute diverticulitis. Am Surg. 1999;65(7):632–635. - PubMed
-
- Francis NK, Sylla P, Abou-Khalil M, Arolfo S, Berler D, Curtis NJ, Dolejs SC, Garfinkle R, Gorter-Stam M, Hashimoto DA, Hassinger TE, Molenaar CJL, Pucher PH, Schuermans V, Arezzo A, Agresta F, Antoniou SA, Arulampalam T, Boutros M, Bouvy N, Campbell K, Francone T, Haggerty SP, Hedrick TL, Stefanidis D, Truitt MS, Kelly J, Ket H, Dunkin BJ, Pietrabissa A. EAES and SAGES 2018 consensus conference on acute diverticulitis management: evidence-based recommendations for clinical practice. Surg Endosc. 2019;33(9):2726–2741. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
