

Risk of Stroke and Bleeding in Atrial Fibrillation Treated with Apixaban Compared with Warfarin
- PMID: 32989717
- PMCID: PMC7728961
- DOI: 10.1007/s11606-020-06180-8
Risk of Stroke and Bleeding in Atrial Fibrillation Treated with Apixaban Compared with Warfarin
Abstract
Background: A previous FDA study reported a favorable benefit risk for apixaban compared with warfarin for stroke prevention in older non-valvular atrial fibrillation (NVAF) patients (≥ 65 years). However, it remains unclear whether this favorable benefit risk persists in other populations including younger users. We examined if a similar benefit risk was observed in the Sentinel System and if it varied by age group.
Objective: To examine the risk of ischemic stroke, gastrointestinal (GI) bleeding, and intracranial hemorrhage (ICH) in apixaban users compared with warfarin users in Sentinel Distributed Database (SDD).
Design and participants: A retrospective new user cohort study was conducted among patients, 21 years and older initiating apixaban and warfarin for NVAF, between December 28, 2012, and June 30, 2018, in the SDD.
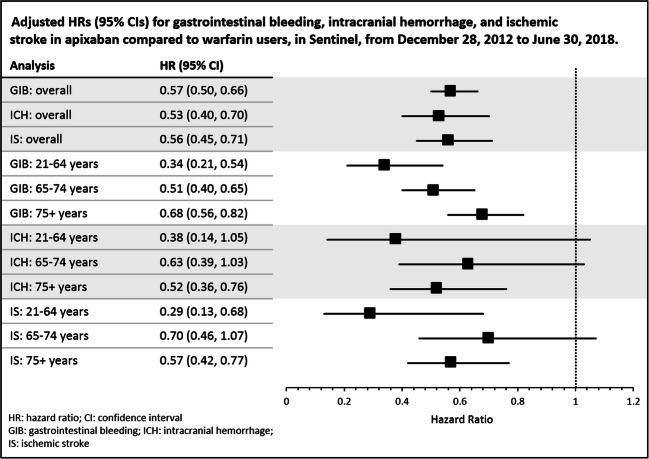
Main measures: Cox proportional hazard regression was used to estimate the hazard ratios (HR) and 95% confidence intervals (95% CI) for each outcome (ischemic stroke, GI bleeding, and ICH) in propensity score matched apixaban users compared with the warfarin users. Subgroup analyses by age (21-64, 65-74, and 75+ years) were conducted.
Key results: After matching, 55.3% and 58.4% (n = 55,038) of the apixaban and warfarin users were included in the main analysis. GI bleeding was the most common outcome. The HR (95% CI) for GI bleeding, ICH, and ischemic stroke in apixaban users compared with warfarin users were 0.57 (0.50-0.66), 0.53 (0.40-0.70), and 0.56 (0.45-0.71) respectively. The reduced risk of these outcomes in apixaban compared with warfarin users persisted across age groups.
Conclusion: In NVAF patients of all ages initiating either apixaban or warfarin for stroke prevention in the Sentinel System, apixaban was associated with a decreased risk of GI bleeding, ICH, and ischemic stroke compared with warfarin. Among patients less than 65 years of age, apixaban use was associated with a decreased risk of GI bleeding and ischemic stroke.
Keywords: Sentinel System; apixaban; bleeding; non-valvular atrial fibrillation; stroke; warfarin.
Conflict of interest statement
The authors declare that they do not have a conflict of interest.
Figures
Similar articles
-
Real-world evidence of stroke prevention in patients with nonvalvular atrial fibrillation in the United States: the REVISIT-US study.Curr Med Res Opin. 2016 Dec;32(12):2047-2053. doi: 10.1080/03007995.2016.1237937. Epub 2016 Sep 20. Curr Med Res Opin. 2016. PMID: 27633045
-
Effectiveness and safety of apixaban versus warfarin in non-valvular atrial fibrillation patients in "real-world" clinical practice. A propensity-matched analysis of 76,940 patients.Thromb Haemost. 2017 Jun 2;117(6):1072-1082. doi: 10.1160/TH17-01-0068. Epub 2017 Mar 16. Thromb Haemost. 2017. PMID: 28300870 Free PMC article.
-
Effectiveness and Safety of Apixaban, Dabigatran, and Rivaroxaban Versus Warfarin in Patients With Nonvalvular Atrial Fibrillation and Previous Stroke or Transient Ischemic Attack.Stroke. 2017 Aug;48(8):2142-2149. doi: 10.1161/STROKEAHA.117.017474. Epub 2017 Jun 27. Stroke. 2017. PMID: 28655814
-
The burden of undertreatment and non-treatment among patients with non-valvular atrial fibrillation and elevated stroke risk: a systematic review.Curr Med Res Opin. 2022 Jan;38(1):7-18. doi: 10.1080/03007995.2021.1982684. Epub 2021 Oct 9. Curr Med Res Opin. 2022. PMID: 34632887
-
Efficacy and safety of apixaban and warfarin in prevention of ischemic stroke: a systematic review and meta-analysis.Arch Med Sci. 2022 Apr 20;21(2):555-563. doi: 10.5114/aoms/148209. eCollection 2025. Arch Med Sci. 2022. PMID: 40395880 Free PMC article. Review.
Cited by
-
Effect of edoxaban compared with other oral anticoagulants for stroke prevention in patients with atrial fibrillation: A meta-analysis.Heliyon. 2023 Nov 3;9(11):e21740. doi: 10.1016/j.heliyon.2023.e21740. eCollection 2023 Nov. Heliyon. 2023. PMID: 38027839 Free PMC article. Review.
-
Effectiveness and Safety of Apixaban in over 3.9 Million People with Atrial Fibrillation: A Systematic Review and Meta-Analysis.J Clin Med. 2022 Jun 30;11(13):3788. doi: 10.3390/jcm11133788. J Clin Med. 2022. PMID: 35807073 Free PMC article. Review.
-
Innovations in pharmacovigilance studies of medicines in older people.Br J Clin Pharmacol. 2025 Jan;91(1):66-83. doi: 10.1111/bcp.16049. Epub 2024 Mar 26. Br J Clin Pharmacol. 2025. PMID: 38529693 Free PMC article. Review.
-
Geographic and Racial Variation in Oral Anticoagulant (OAC) Treatment Among Commercially Insured Patients with Non-valvular Atrial Fibrillation (NVAF) in the United States.Am J Cardiovasc Drugs. 2025 Apr 3. doi: 10.1007/s40256-025-00728-x. Online ahead of print. Am J Cardiovasc Drugs. 2025. PMID: 40178719
-
Reappraisal of Non-vitamin K Antagonist Oral Anticoagulants in Atrial Fibrillation Patients: A Systematic Review and Meta-Analysis.Front Cardiovasc Med. 2021 Oct 15;8:757188. doi: 10.3389/fcvm.2021.757188. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 34722686 Free PMC article.
References
-
- Prevention CfDCa . Atrial fibrillation fact sheet. Atlanta: Centers for Disease Control and Prevention; 2017.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
